

Acellular Dermal Matrix Versus Inferior Deepithelialized Flap Breast Reconstruction: Equivalent Outcomes, with Increased Cost
- PMID: 28740788
- PMCID: PMC5505849
- DOI: 10.1097/GOX.0000000000001382
Acellular Dermal Matrix Versus Inferior Deepithelialized Flap Breast Reconstruction: Equivalent Outcomes, with Increased Cost
Abstract
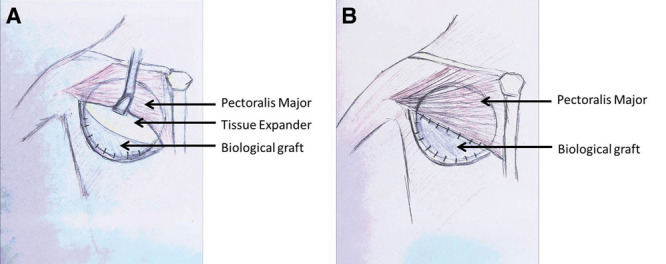
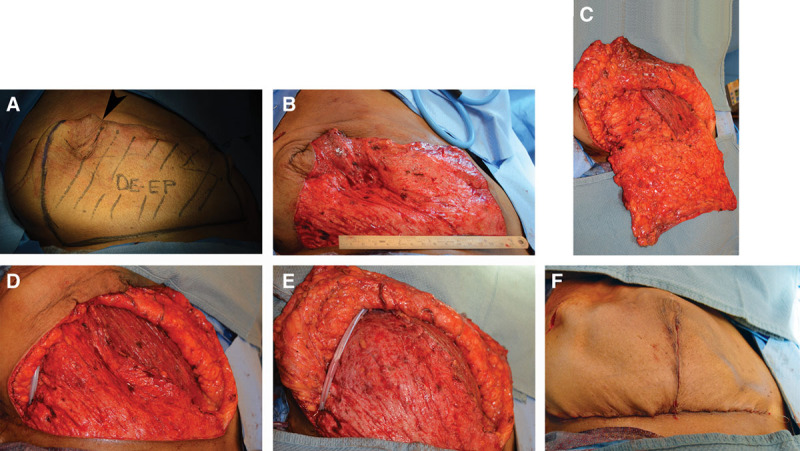
Background: Approximately 250,000 new cases of breast cancer are diagnosed yearly in the U.S. resulting in more postmastectomy breast reconstructions (PMBRs). The acellular dermal matrix (ADM) expander-implant method became popular in the mid-2000s, but newer techniques such as the inferior deepithelialized flap (IDF) has more recently been described. We hypothesize that ADMs and IDFs provide comparable aesthetic outcomes, with no difference in complication rates and operative characteristics.
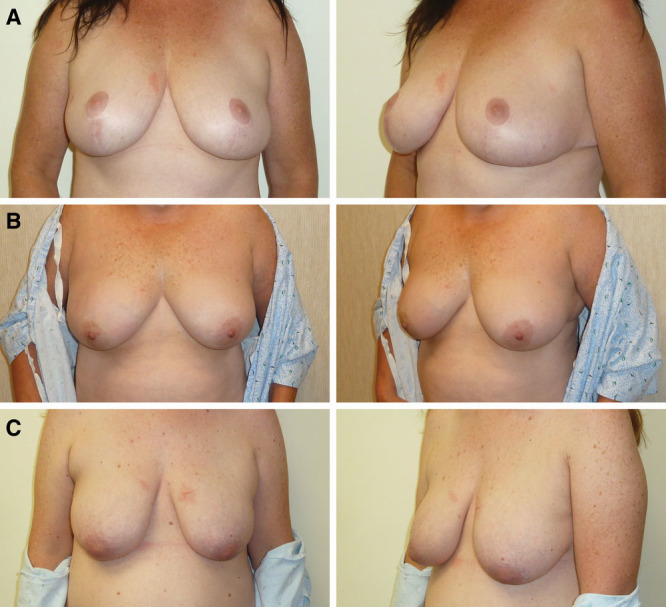
Methods: A retrospective, single-institution study was performed between July 1, 2012, and June 30, 2014, examining all PMBR's (ADM and IDF). Outcomes were categorized as clinical (e.g., complications requiring surgical intervention) or aesthetic.
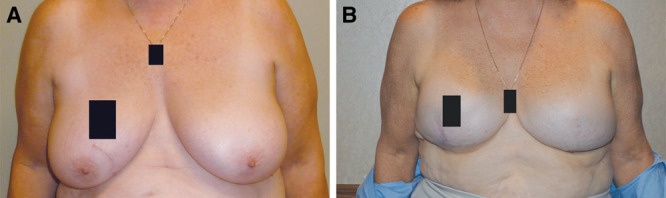
Results: A total of 65 patients (41 ADM; 24 IDF; mean age, 53.4 ± 10.7 years) were included, with 101 PMBR's evaluated (63 ADM and 38 IDF). Patients who underwent IDFs had higher body mass index (32 versus 25; P < 0.01) and higher grades of breast ptosis. Major complication rates were similar between ADM and IDF groups (22% versus 31.5%; P = 0.34). There were no differences in aesthetic outcomes between groups (rater intraclass correlation, 0.92). The average IDF breast reconstruction took nearly 30 minutes longer per reconstructed side (192 minutes versus 166 minutes; P = 0.02), but operative costs were more expensive for the ADM breast reconstruction.
Conclusions: The IDF procedure took 30 minutes longer for each reconstructed side, without significant differences in complications or aesthetic outcomes between the 2 PMBRs. IDF reconstructions may be more suitable for patients with grade 3 breast ptosis and higher body mass index. Further studies should focus on long-term outcomes and value-based approaches to PMBR.
Figures
References
-
- Anderson BO, Yip CH, Ramsey SD, et al. Global Summit Health Care Systems and Public Policy Panel. Breast cancer in limited-resource countries: health care systems and public policy. Breast J. 2006;12:S54–S69. - PubMed
-
- Bouchardy C, Rapiti E, Fioretta G, et al. Undertreatment strongly decreases prognosis of breast cancer in elderly women. J Clin Oncol. 2003;21:3580–3587. - PubMed
-
- Mettlin C.Global breast cancer mortality statistics. CA Cancer J Clin. 1999;49:138–144. - PubMed
-
- breastcancer.org. U.S. breast cancer statistics. 2016. Available at http://www.breastcancer.org/symptoms/understand_bc/statistics. Accessed January 21, 2016.
-
- Dragun AE, Huang B, Tucker TC, et al. Increasing mastectomy rates among all age groups for early stage breast cancer: a 10-year study of surgical choice. Breast J. 2012;18:318–325. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources