

Role of peak current in conversion of patients with ventricular fibrillation
- PMID: 28741007
- PMCID: PMC5523096
- DOI: 10.11622/smedj.2017070
Role of peak current in conversion of patients with ventricular fibrillation
Abstract
Introduction: Peak currents are the final arbiter of defibrillation in patients with ventricular fibrillation (VF). However, biphasic defibrillators continue to use energy in joules for electrical conversion in hopes that their impedance compensation properties will address transthoracic impedance (TTI), which must be overcome when a fixed amount of energy is delivered. However, optimal peak currents for conversion of VF remain unclear. We aimed to determine the role of peak current and optimal peak levels for conversion in collapsed VF patients.
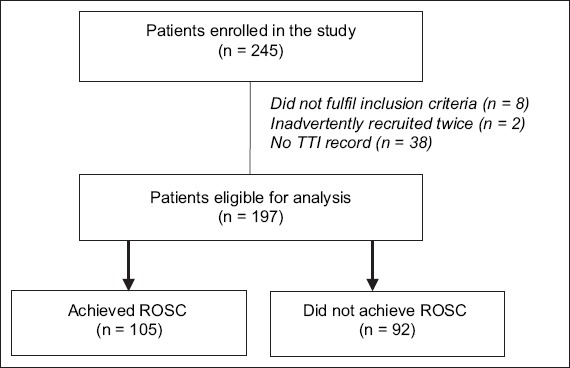
Methods: Adult, non-pregnant patients presenting with non-traumatic VF were included in the study. All defibrillations that occurred were included. Impedance values during defibrillation were used to calculate peak current values. The endpoint was return of spontaneous circulation (ROSC).
Results: Of the 197 patients analysed, 105 had ROSC. Characteristics of patients with and without ROSC were comparable. Short duration of collapse < 10 minutes correlated positively with ROSC. Generally, patients with average or high TTI converted at lower peak currents. 25% of patients with high TTI converted at 13.3 ± 2.3 A, 22.7% with average TTI at 18.2 ± 2.5 A and 18.6% with low TTI at 27.0 ± 4.7 A (p = 0.729). Highest peak current conversions were at < 15 A and 15-20 A. Of the 44 patients who achieved first-shock ROSC, 33 (75.0%) received < 20 A peak current vs. > 20 A for the remaining 11 (25%) patients (p = 0.002).
Conclusion: For best effect, priming biphasic defibrillators to deliver specific peak currents should be considered.
Keywords: collapse duration; defibrillation energy; electrical conversion; peak current; transthoracic impedance.
Copyright: © Singapore Medical Association
Figures
Similar articles
-
Retrospective evaluation of current-based impedance compensation defibrillation in out-of-hospital cardiac arrest.Resuscitation. 2013 May;84(5):580-5. doi: 10.1016/j.resuscitation.2012.09.017. Epub 2012 Sep 20. Resuscitation. 2013. PMID: 23000364
-
Current is better than energy as predictor of success for biphasic defibrillatory shocks in a porcine model of ventricular fibrillation.Resuscitation. 2013 May;84(5):678-83. doi: 10.1016/j.resuscitation.2012.09.029. Epub 2012 Sep 29. Resuscitation. 2013. PMID: 23032689
-
Minimizing pre- and post-defibrillation pauses increases the likelihood of return of spontaneous circulation (ROSC).Resuscitation. 2010 Jul;81(7):822-5. doi: 10.1016/j.resuscitation.2010.03.013. Epub 2010 Apr 15. Resuscitation. 2010. PMID: 20398991
-
A framework of current based defibrillation improves defibrillation efficacy of biphasic truncated exponential waveform in rabbits.Sci Rep. 2021 Jan 15;11(1):1586. doi: 10.1038/s41598-020-80521-9. Sci Rep. 2021. PMID: 33452293 Free PMC article.
-
[Research Progress of External Defibrillation Technique and Its Application].Zhongguo Yi Liao Qi Xie Za Zhi. 2018 May 30;42(3):188-192. doi: 10.3969/j.issn.1671-7104.2018.03.010. Zhongguo Yi Liao Qi Xie Za Zhi. 2018. PMID: 29885126 Review. Chinese.
Cited by
-
[Recent advances in external cardiac defibrillation techniques].Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2020 Dec 25;37(6):1095-1100. doi: 10.7507/1001-5515.202003013. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2020. PMID: 33369350 Free PMC article. Review. Chinese.
-
A Method to Detect Presence of Chest Compressions During Resuscitation Using Transthoracic Impedance.IEEE J Biomed Health Inform. 2020 Mar;24(3):768-774. doi: 10.1109/JBHI.2019.2918790. Epub 2019 May 24. IEEE J Biomed Health Inform. 2020. PMID: 31144648 Free PMC article.
-
A Systematic Review of the Transthoracic Impedance during Cardiac Defibrillation.Sensors (Basel). 2022 Apr 6;22(7):2808. doi: 10.3390/s22072808. Sensors (Basel). 2022. PMID: 35408422 Free PMC article.
-
Combining Ventricular Fibrillation Features With Defibrillation Waveform Parameters Improves the Ability to Predict Shock Outcomes in a Rabbit Model of Cardiac Arrest.J Am Heart Assoc. 2025 Apr;14(7):e039527. doi: 10.1161/JAHA.124.039527. Epub 2025 Mar 27. J Am Heart Assoc. 2025. PMID: 40145324 Free PMC article.
References
-
- Koster RW, Dorian P, Chapman FW, Schmitt PW, O’Grady SG, Walker RG. A randomized trial comparing monophasic and biphasic waveform shocks for external cardioversion of atrial fibrillation. Am Heart J. 2004;147:e20. - PubMed
-
- Niemann JT, Burian D, Garner D, Lewis RJ. Monophasic versus biphasic transthoracic countershock after prolonged ventricular fibrillation in a swine model. J Am Coll Cardiol. 2000;36:932–8. - PubMed
-
- Bardy GH, Marchlinski FE, Sharma AD, et al. Multicenter comparison of truncated biphasic shocks and standard damped sine wave monophasic shocks for transthoracic ventricular defibrillation. Transthoracic Investigators. Circulation. 1996;94:2507–14. - PubMed
-
- Tang W, Weil MH, Sun S, et al. A comparison of biphasic and monophasic waveform defibrillation after prolonged ventricular fibrillation. Chest. 2001;120:948–54. - PubMed
-
- Jain VC, Wheelan K. Successful cardioversion of atrial fibrillation using 360-Joules biphasic shock. Am J Cardiol. 2002;90:331–2. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
