

Subtrochanteric femoral shortening osteotomy combined with cementless total hip replacement for Crowe type IV developmental dysplasia: a retrospective study
- PMID: 28741029
- PMCID: PMC5685984
- DOI: 10.1007/s10195-017-0466-7
Subtrochanteric femoral shortening osteotomy combined with cementless total hip replacement for Crowe type IV developmental dysplasia: a retrospective study
Abstract
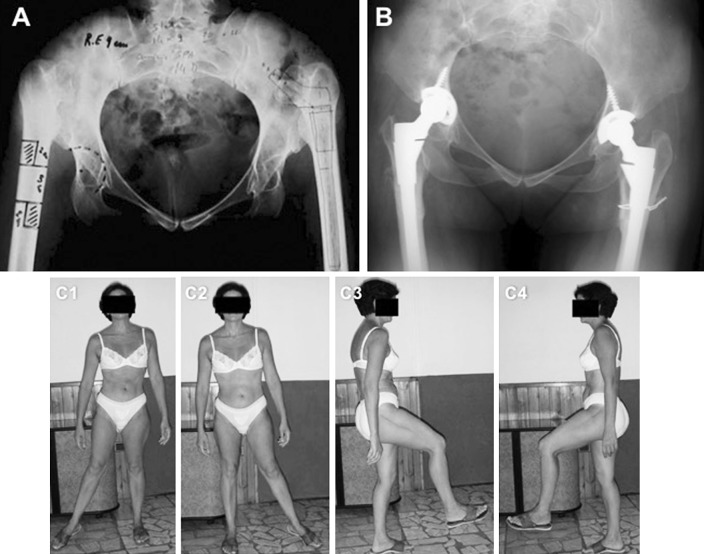
Background: Total hip replacement for high dislocation of the hip presents some difficulties, considering patients' young ages, the abnormal hip anatomy and the high rate of complications. In this study, we present our experience in terms of clinical and radiological results in the treatment of Crowe type IV hips with subtrochanteric femoral shortening osteotomy and cementless total hip replacement.
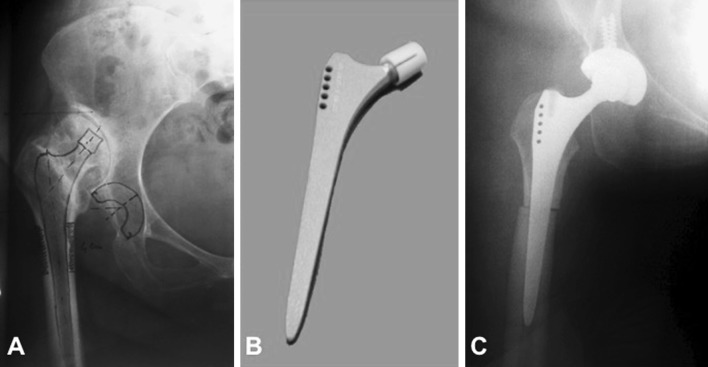
Materials and methods: We retrospectively reviewed 15 patients with Crowe type IV hip dysplasia (two bilateral cases for a total of 17 hips) treated with cementless total hip replacement associated with shortening subtrochanteric osteotomies (nine transversal and eight Z-shape osteotomies) between March 2000 to February 2006. The mean follow-up was 88 months (range 63-133). Harris hip score, leg length discrepancy, neurological status, union status of the osteotomy and the component stability were the criteria of the evaluation. All complications were noted.
Results: The mean HHS improved from 38.3 (range 32-52) to 85.6 (range 69-90). The mean preoperative leg length discrepancy was of 45 mm (range 38-70) and reduced to a mean of 12 mm (range 9-1.6) postoperatively. All osteotomies resulted healed at an average of 12.3 weeks (range 10-15). No cases of delayed union or nonunion were detected. Two patients (11%) showed early symptoms of sciatic nerve palsy which resolved uneventfully in 6 months. There was no migrations and none of the implants required revision.
Conclusions: Cementless THA with shortening subtrochanteric osteotomy is an effective method in the treatment of patients with Crowe type IV development dysplasia of the hip.
Level of evidence: IV.
Keywords: Hip dysplasia; Hip replacement; Shortening osteotomy.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Patient consent
All the patients provided informed consent before being enrolled.
Ethical approval
The study conforms to the 1964 Helsinki Declaration and its later amendments; the responsible Ethics Committee was notified about it.
Funding
The authors declare that no funding was received for this article.
Figures
References
-
- Rosenstein AD, Diaz RJ. Challenges and solutions for total hip arthroplasty in treatment of patients with symptomatic sequelae of developmental dysplasia of the hip. Am J Orthop. 2011;40:87–91. - PubMed
-
- Engesaeter LB, Furnes O, Havelin LI. Developmental dysplasia of the hip-good results of later total hip arthroplasty: 7135 primary total hip arthroplasties after developmental dysplasia of the hip compared with 59774 total hip arthroplasties in idiopathic coxarthrosis followed for 0 to 15 years. J Arthroplast. 2008;23:235–240. doi: 10.1016/j.arth.2007.03.023. - DOI - PubMed
-
- Lewallen DG. Neurovascular injury associated with hip arthroplasty. Instr Course Lect. 1998;47:275–283. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
