

Progesterone receptor modulators for endometriosis
- PMID: 28742263
- PMCID: PMC6483151
- DOI: 10.1002/14651858.CD009881.pub2
Progesterone receptor modulators for endometriosis
Abstract
Background: Endometriosis is defined as the presence of endometrial tissue (glands and stroma) outside the uterine cavity. This condition is oestrogen-dependent and thus is seen primarily during the reproductive years. Owing to their antiproliferative effects in the endometrium, progesterone receptor modulators (PRMs) have been advocated for treatment of endometriosis.
Objectives: To assess the effectiveness and safety of PRMs primarily in terms of pain relief as compared with other treatments or placebo or no treatment in women of reproductive age with endometriosis.
Search methods: We searched the following electronic databases, trial registers, and websites: the Cochrane Gynaecology and Fertility Group (CGFG) Specialised Register of Controlled Trials, the Central Register of Studies Online (CRSO), MEDLINE, Embase, PsycINFO, clinicaltrials.gov, and the World Health Organization (WHO) platform, from inception to 28 November 2016. We handsearched reference lists of articles retrieved by the search.
Selection criteria: We included randomised controlled trials (RCTs) published in all languages that examined effects of PRMs for treatment of symptomatic endometriosis.
Data collection and analysis: We used standard methodological procedures as expected by the Cochrane Collaboration. Primary outcomes included measures of pain and side effects.
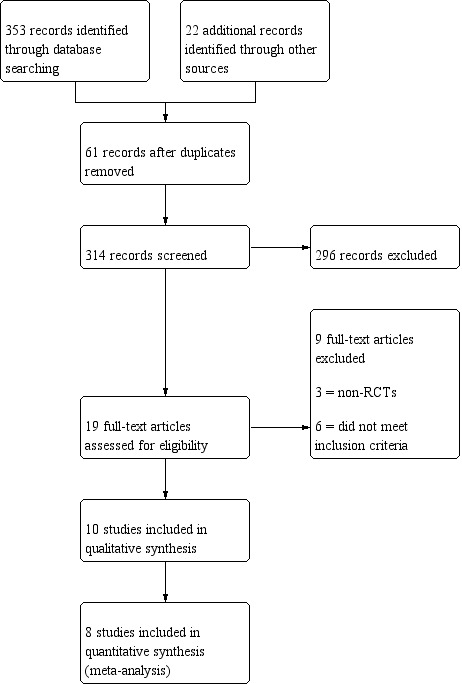
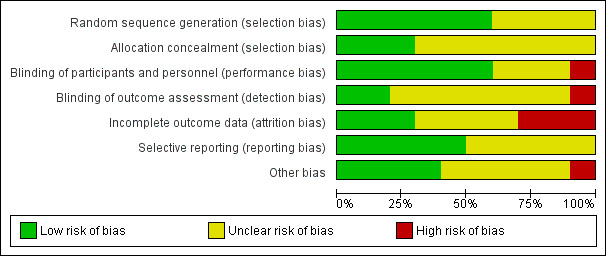
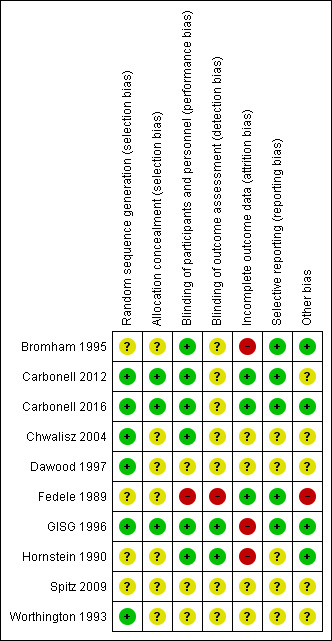
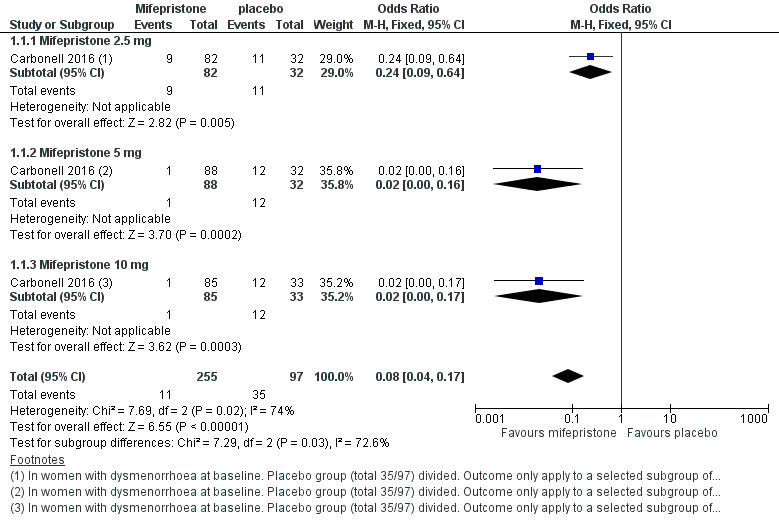
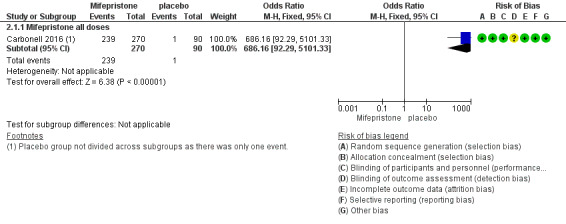
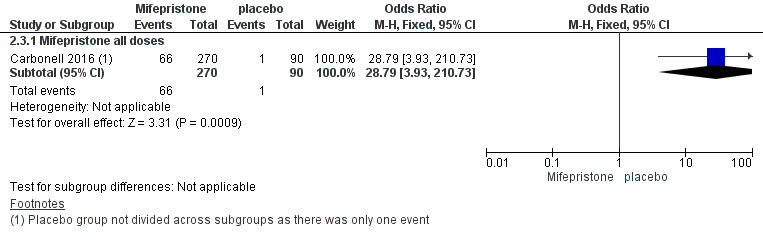
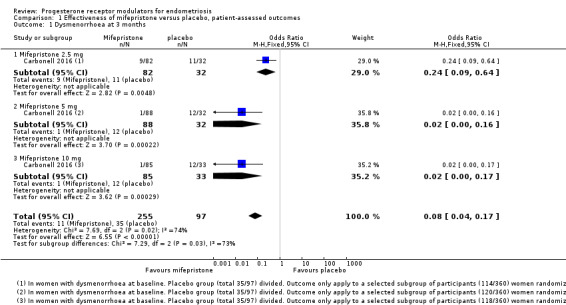
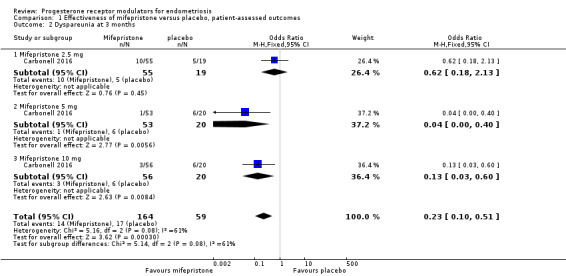
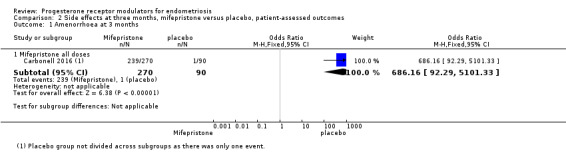
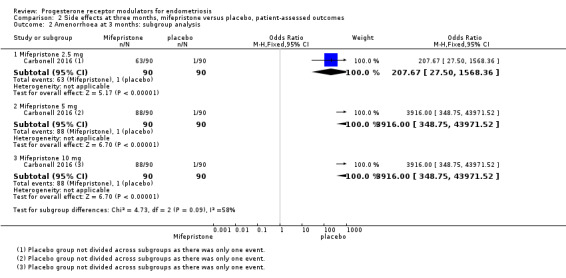
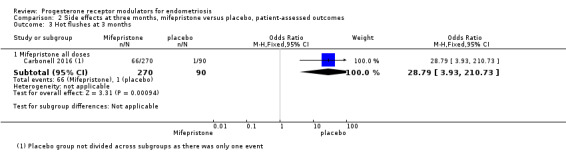
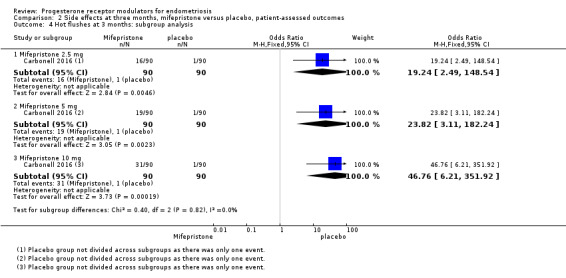
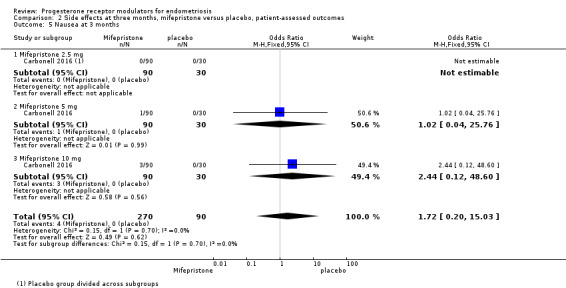
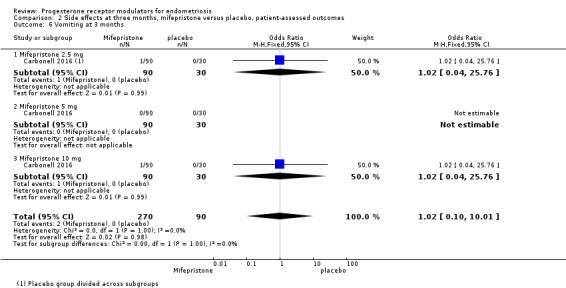
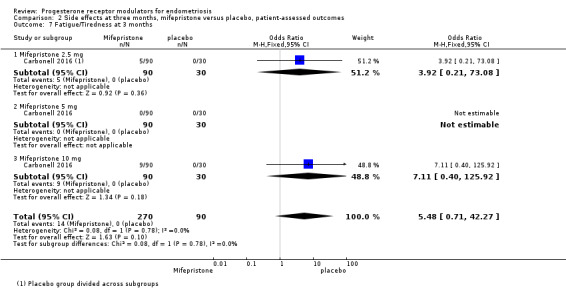
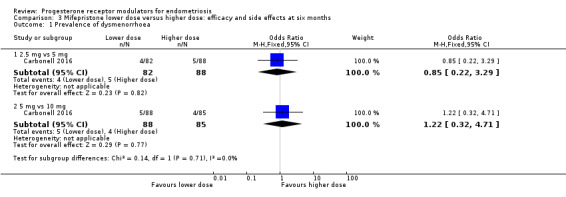
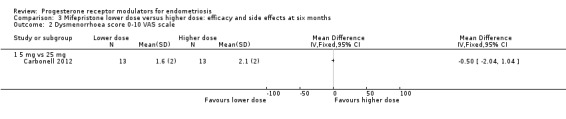
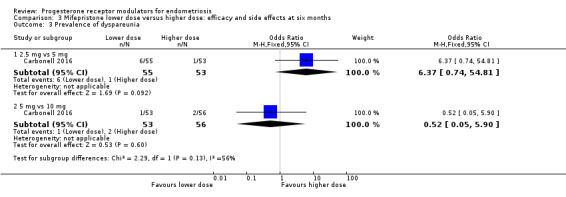
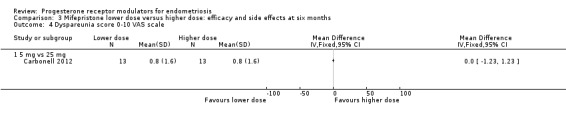
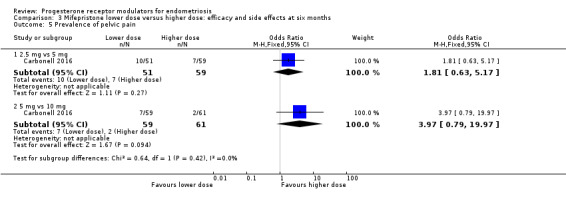
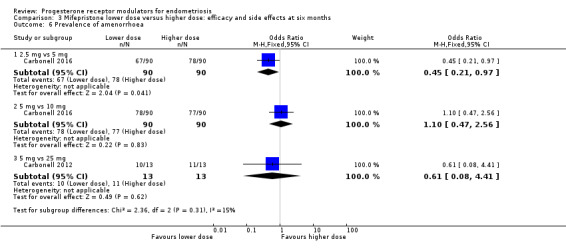
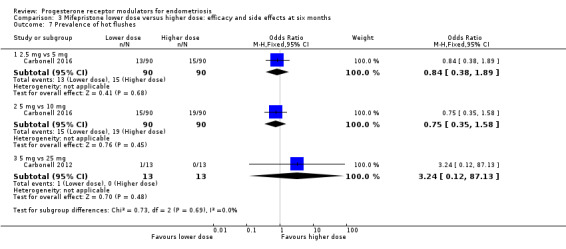
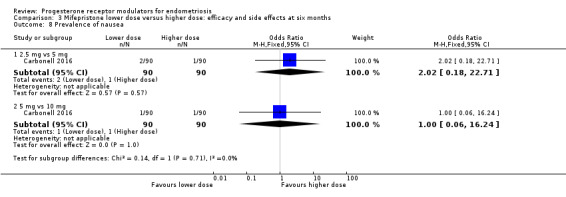
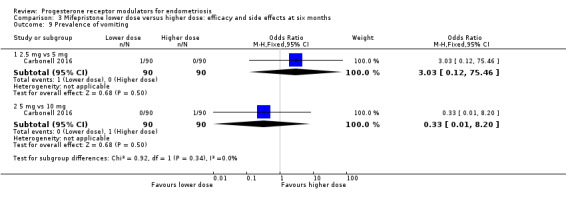
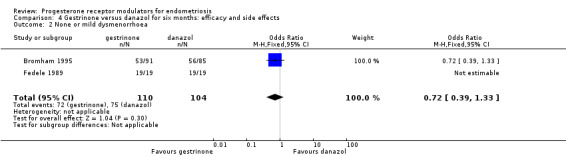
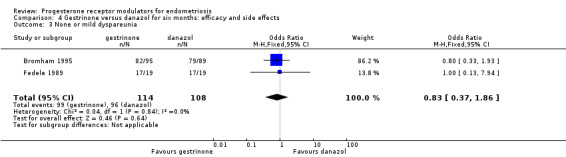
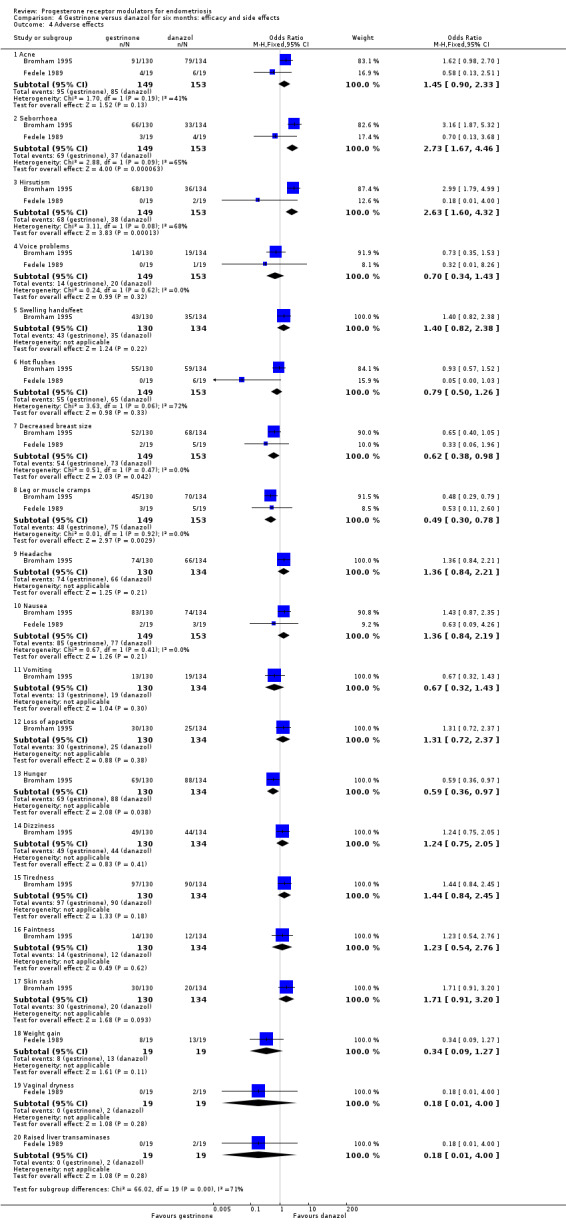
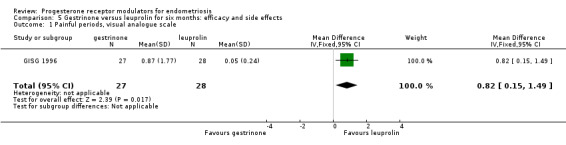
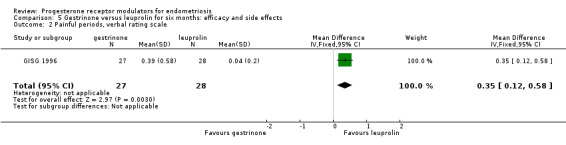
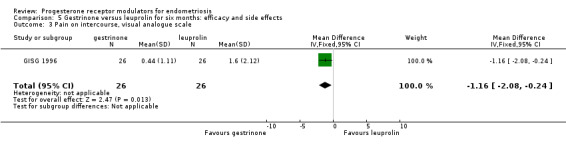
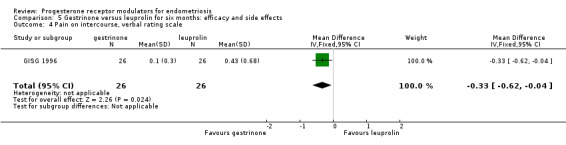
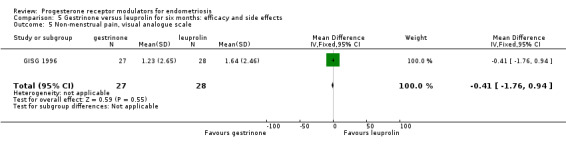
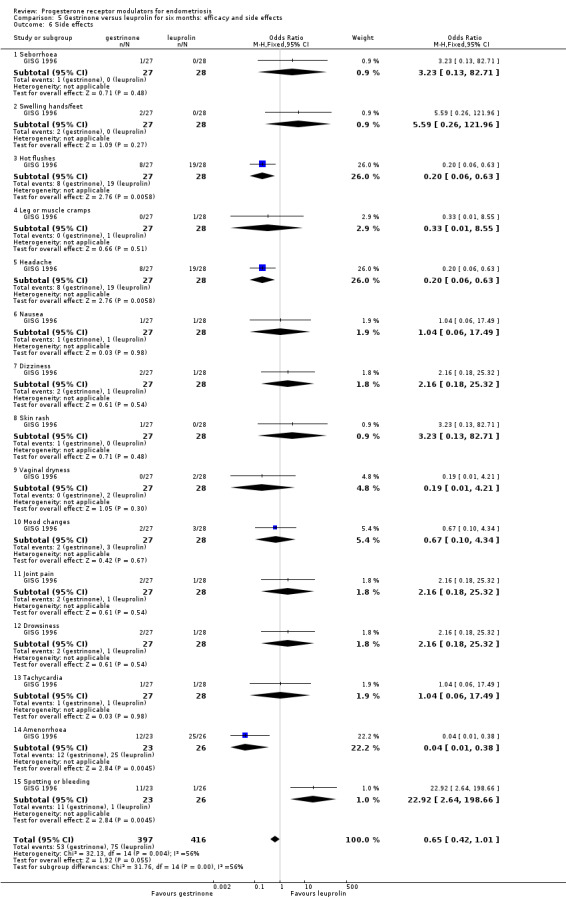
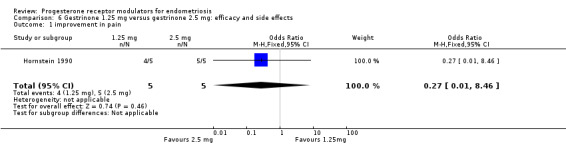
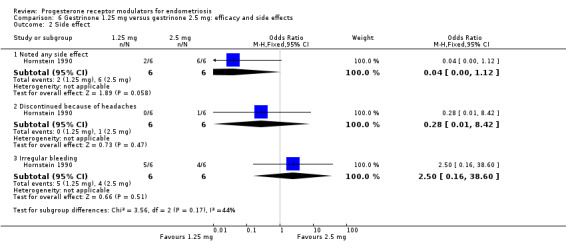
Main results: We included 10 randomised controlled trials (RCTs) with 960 women. Two RCTs compared mifepristone versus placebo or versus a different dose of mifepristone, one RCT compared asoprisnil versus placebo, one compared ulipristal versus leuprolide acetate, and four compared gestrinone versus danazol, gonadotropin-releasing hormone (GnRH) analogues, or a different dose of gestrinone. The quality of evidence ranged from high to very low. The main limitations were serious risk of bias (associated with poor reporting of methods and high or unclear rates of attrition in most studies), very serious imprecision (associated with low event rates and wide confidence intervals), and indirectness (outcome assessed in a select subgroup of participants). Mifepristone versus placebo One study made this comparison and reported rates of painful symptoms among women who reported symptoms at baseline.At three months, the mifepristone group had lower rates of dysmenorrhoea (odds ratio (OR) 0.08, 95% confidence interval (CI) 0.04 to 0.17; one RCT, n =352; moderate-quality evidence), suggesting that if 40% of women taking placebo experience dysmenorrhoea, then between 3% and 10% of women taking mifepristone will do so. The mifepristone group also had lower rates of dyspareunia (OR 0.23, 95% CI 0.11 to 0.51; one RCT, n = 223; low-quality evidence). However, the mifepristone group had higher rates of side effects: Nearly 90% had amenorrhoea and 24% had hot flushes, although the placebo group reported only one event of each (1%) (high-quality evidence). Evidence was insufficient to show differences in rates of nausea, vomiting, or fatigue, if present. Mifepristone dose comparisons Two studies compared doses of mifepristone and found insufficient evidence to show differences between different doses in terms of effectiveness or safety, if present. However, subgroup analysis of comparisons between mifepristone and placebo suggest that the 2.5 mg dose may be less effective than 5 mg or 10 mg for treating dysmenorrhoea or dyspareunia. Gestrinone comparisons Ons study compared gestrinone with danazol, and another study compared gestrinone with leuprolin.Evidence was insufficient to show differences, if present, between gestrinone and danazol in rate of pain relief (those reporting no or mild pelvic pain) (OR 0.71, 95% CI 0.33 to 1.56; two RCTs, n = 230; very low-quality evidence), dysmenorrhoea (OR 0.72, 95% CI 0.39 to 1.33; two RCTs, n = 214; very low-quality evidence), or dyspareunia (OR 0.83, 95% CI 0.37 to 1.86; two RCTs, n = 222; very low-quality evidence). The gestrinone group had a higher rate of hirsutism (OR 2.63, 95% CI 1.60 to 4.32; two RCTs, n = 302; very low-quality evidence) and a lower rate of decreased breast size (OR 0.62, 95% CI 0.38 to 0.98; two RCTs, n = 302; low-quality evidence). Evidence was insufficient to show differences between groups, if present, in rate of hot flushes (OR 0.79, 95% CI 0.50 to 1.26; two RCTs, n = 302; very low-quality evidence) or acne (OR 1.45, 95% CI 0.90 to 2.33; two RCTs, n = 302; low-quality evidence).When researchers compared gestrinone versus leuprolin through measurements on the 1 to 3 verbal rating scale (lower score denotes benefit), the mean dysmenorrhoea score was higher in the gestrinone group (MD 0.35 points, 95% CI 0.12 to 0.58; one RCT, n = 55; low-quality evidence), but the mean dyspareunia score was lower in this group (MD 0.33 points, 95% CI 0.62 to 0.04; low-quality evidence). The gestrinone group had lower rates of amenorrhoea (OR 0.04, 95% CI 0.01 to 0.38; one RCT, n = 49; low-quality evidence) and hot flushes (OR 0.20, 95% CI 0.06 to 0.63; one study, n = 55; low quality evidence) but higher rates of spotting or bleeding (OR 22.92, 95% CI 2.64 to 198.66; one RCT, n = 49; low-quality evidence).Evidence was insufficient to show differences in effectiveness or safety between different doses of gestrinone, if present. Asoprisnil versus placebo One study (n = 130) made this comparison but did not report data suitable for analysis. Ulipristal versus leuprolide acetate One study (n = 38) made this comparison but did not report data suitable for analysis.
Authors' conclusions: Among women with endometriosis, moderate-quality evidence shows that mifepristone relieves dysmenorrhoea, and low-quality evidence suggests that this agent relieves dyspareunia, although amenorrhoea and hot flushes are common side effects. Data on dosage were inconclusive, although they suggest that the 2.5 mg dose of mifepristone may be less effective than higher doses. We found insufficient evidence to permit firm conclusions about the safety and effectiveness of other progesterone receptor modulators.
Conflict of interest statement
JF, HS, MZ, HZ, YW, HC and WH have no interests to declare.
Figures





Update of
References
References to studies included in this review
Bromham 1995 {published data only}
-
- Bromham DR, Booker MW, Rose GL, Wardle PG, Newton JR. A multicentre comparative study of gestrinone and danazol in the treatment of endometriosis. Journal of Obstetrics and Gynaecology 1995;15:188‐94.
-
- Bromham DR, Booker MW, Rose GL, Wardle PG, Newton JR. Updating the clinical experience in endometriosis ‐ the European perspective. British Journal of Obstetrics and Gynaecology 1995;102 Suppl 12:12‐6. - PubMed
Carbonell 2012 {published data only}
-
- Carbonell JL, Perera O, Riveron AM, Giuseppe JG. Treatment with 5 mg or 25 mg of mifepristone daily for six months. A randomized double‐blind study [Tratamiento de la endometriosis con 5 mg o 25 mg diariosde mifepristona durante 6 meses. Ensayo clı ´nico aleatorizado,doble ciego]. Progresos de Obstetricia y Ginecologia 2012;55(2):51‐9.
Carbonell 2016 {published data only}
-
- Carbonell JL, Riveron AM, Leonard Y, González J, Heredia B, Sánchez C. Mifepristone 2.5, 5, 10 mg versus placebo in the treatment of endometriosis. Journal of Reproductive Health and Medicine 2016;2:17‐25.
Chwalisz 2004 {published data only}
-
- Chwalisz K, Perez MC, Demanno D, Winkel C, Schubert G, Elger W. Treatment of endometriosis with the novel selective progesterone receptor modulator (SPRM) asoprisnil. Fertility and Sterility 2004;82(Suppl 2):S83‐4.
Dawood 1997 {published data only}
-
- Dawood MY, Obasiolu CW, Ramos J, Khan‐Dawood FS. Clinical, endocrine, and metabolic effects of two doses of gestrinone in treatment of pelvic endometriosis. American Journal of Obstetrics and Gynecology 1997;176(2):387‐94. - PubMed
Fedele 1989 {published data only}
-
- Fedele L, Arcaini L, Bianchi S, Viezzoli T, Arcaini L, Candiani GB. Gestrinone versus danazol in the treatment of endometriosis. Fertility and Sterility 1989;51:781‐5. - PubMed
GISG 1996 {published data only}
-
- Gestrinone Italian Study Group. Gestrinone versus a gonadotropin releasing hormone agonist for the treatment of pelvic pain associated with endometriosis: a multicenter, randomised, double‐blind study. Fertility and Sterility 1996;66:911‐9. - PubMed
Hornstein 1990 {published data only}
-
- Hornstein MD, Glaeson RE, Barbieri RL. A randomised, double‐blind prospective trial of two doses of gestrinone in the treatment of endometriosis. Fertility and Sterility 1990;53:237‐41. - PubMed
Spitz 2009 {published data only}
-
- Spitz IM. Clinical utility of progesterone receptor modulators and their effect on the endometrium. Current Opinion in Obstetrics and Gynecology 2009;21:318‐24. - PubMed
-
- Spitz IM, Wiehle RD, Van AA. Progesterone receptor modulators in endometriosis: a new therapeutic option. In: Garcia‐Velasco J, Rizk B editor(s). Textbook of Endometriosis. India: Jaypee Brothers Medical Publishers Ltd, 2009.
Worthington 1993 {published data only}
-
- Worthington M, Irvine LM, Crook D, Lees B, Shaw RW, Stevenson JC. A randomized comparative study of the metabolic effects of two regimens of gestrinone in the treatment of endometriosis. Fertility and Sterility 1993;59(3):522‐6. - PubMed
References to studies excluded from this review
Bulun 2016 {unpublished data only}
-
- Bulun S. Ulipristal for endometriosis‐related pelvic pain. ClinicalTrials.gov Identifier:NCT02213081 This study is ongoing but is not recruiting participants.
Kettel 1996 {published data only}
-
- Kettel L, Murphy A, Morales A, Ulmann A, Baulieu EE, Yen SS. Treatment of endometriosis with the antiprogesterone mifepristone (RU486). Fertility and Sterility 1996;65(1):23‐8. - PubMed
Kettel 1998 {published data only}
-
- Kettel LM, Murphy AA, Morales AJ, Yen SS. Preliminary report on the treatment of endometriosis with low dose mifepristone (RU 486). American Journal of Obstetrics and Gynecology 1998;178:1151‐6.. - PubMed
Mettler 1987 {published data only}
-
- Mettler L, Semm K. Three‐step therapy of genital endometriosis in cases of human infertility with lynestrenol, danazol or gestrinone administration in the second step. In: Raynaud JP editor(s). Medical Management of Endometriosis. New York: Raven Press, 1984:33‐47.
Nieto 1996 {published data only}
-
- Nieto A, Tacuri C, Serra M, Keller J, Cortes‐Prieto J. Long term follow‐up of endometriosis after two different therapies (gestrinone and buserelin). Clinical & Experimental Obstetrics and Gynecology 1996;23:199‐203. - PubMed
Nobel 1980 {published data only}
-
- Noble AD, Letchworth AT. Treatment of endometriosis: a study of medical management. British Journal of Obstetrics and Gynaecology 1980;87:726‐8. - PubMed
Thomas 1987 {published data only}
Yang 2006 {published data only}
-
- Yang D, Ma W, Qu F, Ma B. Comparative study of Yiweining and gestrinone for post‐operational treatment of stage 3 endometriosis. Chinese Journal of Integrative Medicine 2006;12(3):218‐20. - PubMed
Zhang 2016 {published data only}
-
- Zhang YX. Effect of mifepristone in the different treatments of endometriosis. Clinical & Experimental Obstetrics and Gynecology 2016;43(3):350‐3. - PubMed
Additional references
Berek 2007
-
- Berek JS. Endometriosis. Berek & Novak's Gynecology. 14. Baltimore, MD: Lippincott Williams & Wilkins, 2007.
Bouchard 2011
-
- Bouchard P, Chabbert BN, Fauser BC. Selective progesterone receptor modulators in reproductive medicine: pharmacology, clinical efficacy and safety. Fertility and Sterility 2011;96:1175‐89. - PubMed
Brenner 2002
-
- Brenner RM, Slayden OD, Critchley HO. Anti‐proliferative effects of progesterone antagonists in the primate endometrium: a potential role for the androgen receptor. Reproduction 2002;124(2):167‐72. - PubMed
Brenner 2005
-
- Brenner RM, Slayden OD. Progesterone receptor antagonists and the endometrial antiproliferative effect. Seminars in Reproductive Medicine 2005;23(1):74‐81. - PubMed
Brown 2002
-
- Brown A, Cheng L, Lin S, Baird DT. Daily low‐dose mifepristone has contraceptive potential by suppressing ovulation and menstruation: a double‐blind randomized control trial of 2 and 5 mg per day for 120 days. Journal of Clinical Endocrinology and Metabolism 2002;87(1):63‐70. - PubMed
Brown 2014
Cramer 2002
-
- Cramer D, Missmer S. The epidemiology of endometriosis. Annals of the New York Academy of Sciences 2002;955:11‐22. - PubMed
Eskenazi 1997
-
- Eskenazi B, Warner M. Epidemiology of endometriosis. Obstetrics and Gynecology Clinics of North America 1997;24:235‐58. - PubMed
Giudice 2010
Goldstein 1980
-
- Goldstein DP, deCholnoky C, Emans SJ, Leventhal JM. Laparoscopy in the diagnosis and management of pelvic pain in adolescents. Journal of Reproductive Medicine 1980;24:251‐6. - PubMed
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. www.cochrane‐handbook.org. Wiley.
Koide 1998
-
- Koide S. Mifepristone: auxiliary therapeutic use in cancer and related disorders. Journal of Reproductive Medicine 1998;43:551‐60. - PubMed
Li 2016
-
- Li W, Li X, Zhang B, Gao C, Chen Y, Jiang Y. Current progresses and trends in the development of progesterone receptor modulators. Current Medicinal Chemistry 2016;23:2507‐54. - PubMed
Mahutte 2003
-
- Mahutte NG, Arici A. Medical management of endometriosis‐associated pain. Obstetrics & Gynecology Clinics of North America 2003;30:133‐50. - PubMed
Narvekar 2004
-
- Narvekar N, Cameron S, Critchley HO, Lin S, Cheng L, Baird DT. Low‐dose mifepristone inhibits endometrial proliferation and up‐regulates androgen receptor. Journal of Clinical Endocrinology & Metabolism 2004;89(5):2491‐7. - PubMed
Neulen 1996
-
- Neulen J, Williams RF, Breckwoldt M, Chwalisz K, Baulieu EE, Hodgen GD. Non‐competitive anti‐oestrogenic actions of progesterone antagonists in primate endometrium: enhancement of oestrogen and progesterone receptors with blockade of post‐receptor proliferative mechanisms. Human Reproduction 1996;11:1533‐7. - PubMed
Sampson 1927
-
- Sampson J. Peritoneal endometriosis due to menstrual dissemination of endometrial tissue into the pelvic cavity. American Journal of Obstetrics and Gynecology 1927;14:422‐69.
Spitz 2003
-
- Spitz IM. Progesterone antagonists and progesterone receptor modulators: an overview. Steroids 2003;68:981‐93. - PubMed
Tosti 2016
-
- Tosti C, Biscione A, Morgante G, Bifulco G, Luisi S, Petraglia F. Hormonal therapy for endometriosis: from molecular research to bedside. European Journal of Obstetrics & Gynecology and Reproductive Biology 2016;5:32. - PubMed
Vercellini 2014
-
- Vercellini P, Viganò P, Somigliana E, Fedele L. Endometriosis: pathogenesis and treatment. Nature Reviews Endocrinology 2014;10:261‐75. - PubMed
Williams 2007
-
- Williams AR, Critchley HO, Osei J, Ingamells S, Cameron IT, Han C. The effects of the selective progesterone receptor modulator asoprisnil on the morphology of uterine tissues after 3 months treatment in patients with symptomatic uterine leiomyomata. Human Reproduction 2007;22(6):1696‐704. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials