

Prognostic factors and survival outcomes in patients with chronic myeloid leukemia in blast phase in the tyrosine kinase inhibitor era: Cohort study of 477 patients
- PMID: 28743165
- PMCID: PMC5673547
- DOI: 10.1002/cncr.30864
Prognostic factors and survival outcomes in patients with chronic myeloid leukemia in blast phase in the tyrosine kinase inhibitor era: Cohort study of 477 patients
Abstract
Background: Outcomes in patients with chronic myeloid leukemia in blast phase (CML-BP) are historically dismal. Herein, the authors sought to analyze the characteristics, prognostic factors, and survival outcomes in patients with CML-BP in the tyrosine kinase inhibitor (TKI) era.
Methods: A total of 477 patients with CML-BP were treated with a TKI at some point during the course of their CML. Cox proportional hazard models identified characteristics that were predictive of survival. Overall survival and failure-free survival were assessed. Optimal cutoff points for specific parameters were identified using classification and regression tree (CART) analysis.
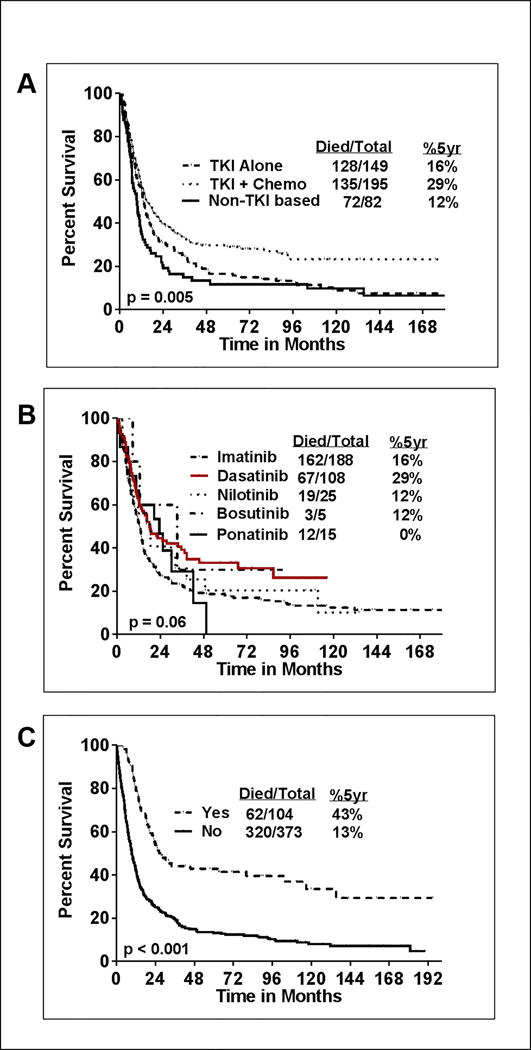
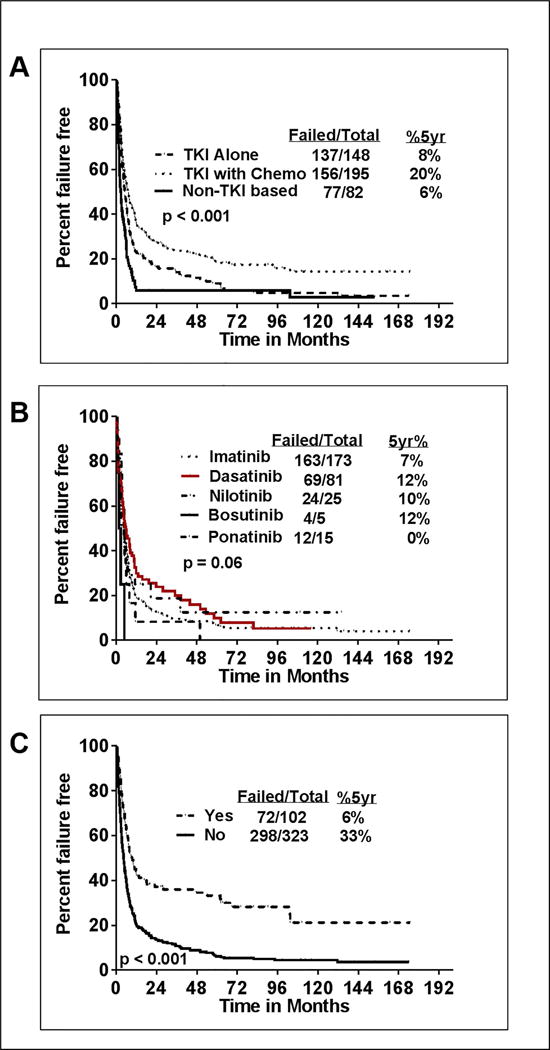
Results: The median age of the patients was 53 years (range, 16-84 years) and 64% were male. Approximately 80% of patients initially were diagnosed in the chronic phase of CML at a median of 41 months (range, 0.7-298 months) before transformation to CML-BP. De novo CML-BP occurred in 71 patients. Approximately 72% of patients received TKI therapy before CML-BP. The initial therapy for CML-BP included a TKI alone (35%), a TKI with chemotherapy (46%), and non-TKI therapies (19%). The median overall survival was 12 months and the median failure-free survival was 5 months. In multivariate analysis, myeloid immunophenotype, prior TKI, age ≥58 years, lactate dehydrogenase level ≥1227 IU/L, platelet count < 102 K/μL, no history of stem cell transplantation, transition to BP from chronic phase/accelerated phase, and the presence of chromosome 15 aberrations predicted for a significantly increased risk of death. Achievement of major hematologic response and/or complete cytogenetic response to first-line treatment was found to be predictive of better survival. The combination of a TKI with intensive chemotherapy followed by stem cell transplantation appeared to confer the best outcome.
Conclusions: Patients with CML-BP continue to pose a therapeutic challenge, have dismal outcomes, and require newer treatment approaches. Cancer 2017;123:4391-402. © 2017 American Cancer Society.
Keywords: blast phase (BP); bosutinib; chronic myeloid leukemia (CML); dasatinib; imatinib; nilotinib; ponatinib; tyrosine kinase inhibitors (TKI).
© 2017 American Cancer Society.
Conflict of interest statement
Figures

References
-
- Hoffmann VS, Baccarani M, Hasford J, et al. The EUTOS population-based registry: incidence and clinical characteristics of 2904 CML patients in 20 European Countries. Leukemia. 2015;29(6):1336–1343. - PubMed
-
- Perez-Jacobo F, Tuna-Aguilar E, Demichelis-Gomez R, et al. Prognostic Factors, Response to Treatment, and Survival in Patients With Chronic Myeloid Leukemia in Blast Phase: A Single-Institution Survey. Clin Lymphoma Myeloma Leuk. 2015;15(12):778–784. - PubMed
-
- Hehlmann R, Saussele S, Voskanyan A, Silver RT. Management of CML-blast crisis. Best Pract Res Clin Haematol. 2016;29(3):295–307. - PubMed
-
- Kantarjian HM, Keating MJ, Talpaz M, et al. Chronic myelogenous leukemia in blast crisis. Analysis of 242 patients. Am J Med. 1987;83(3):445–454. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
