

Gut microbiota and IBD: causation or correlation?
- PMID: 28743984
- PMCID: PMC5880536
- DOI: 10.1038/nrgastro.2017.88
Gut microbiota and IBD: causation or correlation?
Abstract
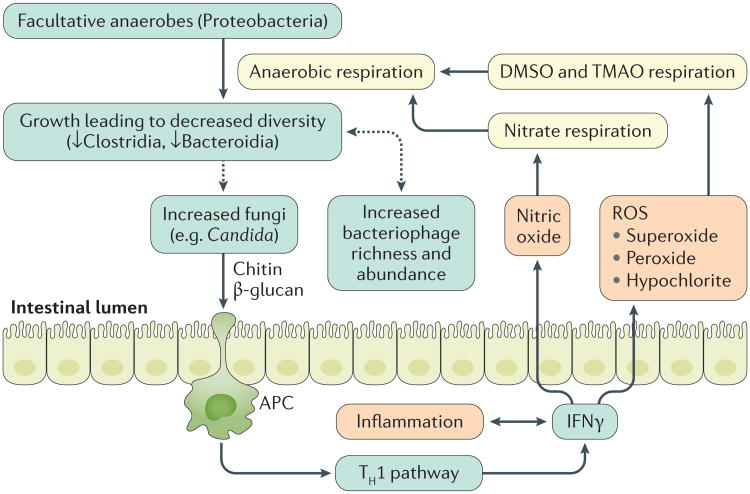
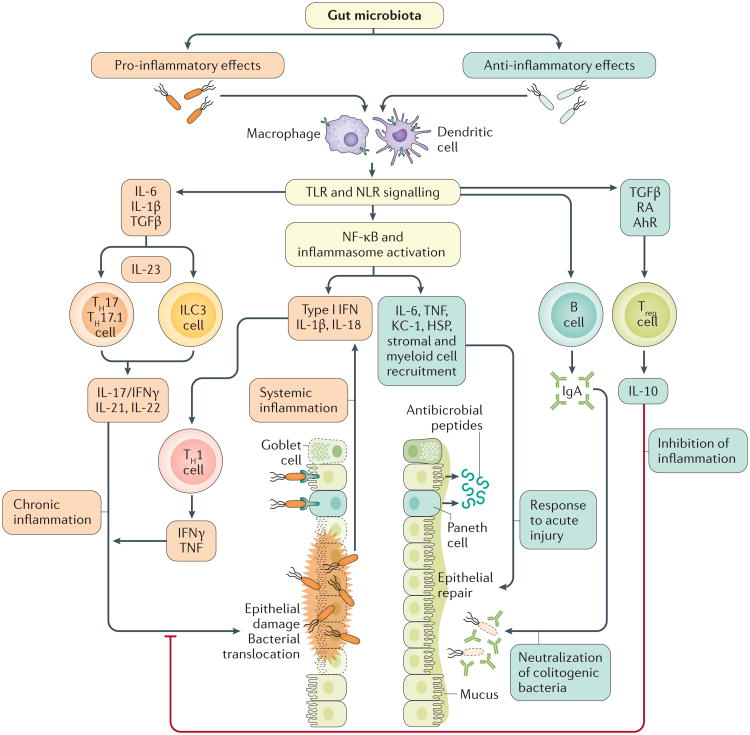
A general consensus exists that IBD is associated with compositional and metabolic changes in the intestinal microbiota (dysbiosis). However, a direct causal relationship between dysbiosis and IBD has not been definitively established in humans. Findings from animal models have revealed diverse and context-specific roles of the gut microbiota in health and disease, ranging from protective to pro-inflammatory actions. Moreover, evidence from these experimental models suggest that although gut bacteria often drive immune activation, chronic inflammation in turn shapes the gut microbiota and contributes to dysbiosis. The purpose of this Review is to summarize current associations between IBD and dysbiosis, describe the role of the gut microbiota in the context of specific animal models of colitis, and discuss the potential role of microbiota-focused interventions in the treatment of human IBD. Ultimately, more studies will be needed to define host-microbial relationships relevant to human disease and amenable to therapeutic interventions.
Figures
References
-
- Dahlhamer JM, Zammitti EP, Ward BW, Wheaton AG, Croft JB. Prevalence of inflammatory bowel disease among adults aged ≥18 Years — United States, 2015. MMWR Morb Mortal Wkly Rep. 2016;65:1166–1169. - PubMed
-
- Molodecky NA, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142:46–54.e42. - PubMed
-
- Manichanh C, Borruel N, Casellas F, Guarner F. The gut microbiota in IBD. Nat Rev Gastroenterol Hepatol. 2012;9:599–608. - PubMed
-
- Sartor RB, Mazmanian SK. Intestinal microbes in inflammatory bowel diseases. Am J Gastroenterol Suppl. 2012;1:15–21.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
