

Pelvic radiograph in skeletal dysplasias: An approach
- PMID: 28744080
- PMCID: PMC5510317
- DOI: 10.4103/ijri.IJRI_367_16
Pelvic radiograph in skeletal dysplasias: An approach
Abstract
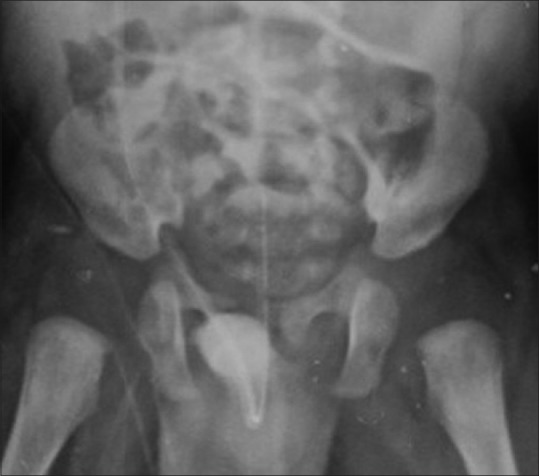
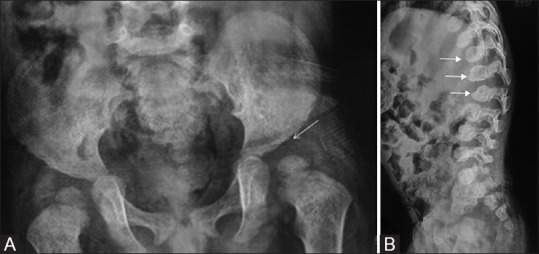
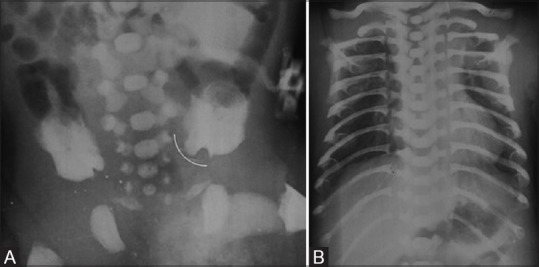
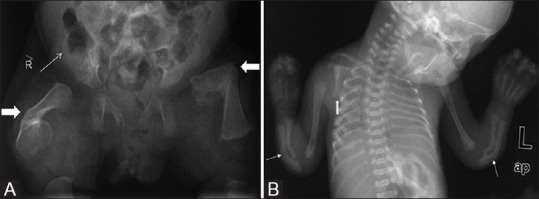
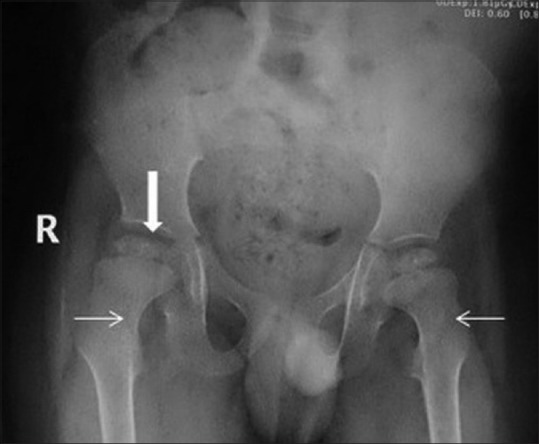
The bony pelvis is constituted by the ilium, ischium, pubis, and sacrum. The pelvic radiograph is an important component of the skeletal survey performed in suspected skeletal dysplasia. Most of the common skeletal dysplasias have either minor or major radiological abnormalities; hence, knowledge of the normal radiological appearance of bony pelvis is vital for recognizing the early signs of various skeletal dysplasias. This article discusses many common and some uncommon radiological findings on pelvic radiographs along with the specific dysplasia in which they are seen; common differential diagnostic considerations are also discussed.
Keywords: Achondroplasia; pelvic radiograph; skeletal dysplasia.
Conflict of interest statement
There are no conflicts of interest.
Figures

















Similar articles
-
The Radiograph of the Pelvis as a Window to Skeletal Dysplasias.Indian J Pediatr. 2016 Jun;83(6):543-52. doi: 10.1007/s12098-015-1919-8. Epub 2016 Jan 29. Indian J Pediatr. 2016. PMID: 26821546 Review.
-
Skeletal dysplasias: A radiographic approach and review of common non-lethal skeletal dysplasias.World J Radiol. 2014 Oct 28;6(10):808-25. doi: 10.4329/wjr.v6.i10.808. World J Radiol. 2014. PMID: 25349664 Free PMC article. Review.
-
Pediatric pelvis: radiographic appearance in various congenital disorders.Radiographics. 1992 May;12(3):467-84. doi: 10.1148/radiographics.12.3.1609139. Radiographics. 1992. PMID: 1609139 Review.
-
Spine radiograph in dysplasias: A pictorial essay.Indian J Radiol Imaging. 2020 Oct-Dec;30(4):436-447. doi: 10.4103/ijri.IJRI_395_20. Epub 2021 Jan 13. Indian J Radiol Imaging. 2020. PMID: 33737772 Free PMC article.
-
Avian pelvis originates from lateral plate mesoderm and its development requires signals from both ectoderm and paraxial mesoderm.Cell Tissue Res. 2008 Mar;331(3):595-604. doi: 10.1007/s00441-007-0556-6. Epub 2007 Dec 18. Cell Tissue Res. 2008. PMID: 18087724
Cited by
-
Quantitative anatomy of the ilium's primary ossification center in the human fetus.Surg Radiol Anat. 2018 Sep;40(9):1047-1054. doi: 10.1007/s00276-018-2018-0. Epub 2018 Apr 19. Surg Radiol Anat. 2018. PMID: 29675677 Free PMC article.
-
Quantitative anatomy of the ulna's shaft primary ossification center in the human fetus.Surg Radiol Anat. 2019 Apr;41(4):431-439. doi: 10.1007/s00276-018-2121-2. Epub 2018 Oct 31. Surg Radiol Anat. 2019. PMID: 30382328 Free PMC article.
-
The pelvic radiograph: lines, arcs and stripes.Singapore Med J. 2021 Jul;62(7):333-340. doi: 10.11622/smedj.2021091. Singapore Med J. 2021. PMID: 34409477 Free PMC article. No abstract available.
-
Morphometric study of the primary ossification center of the fibular shaft in the human fetus.Surg Radiol Anat. 2019 Mar;41(3):297-305. doi: 10.1007/s00276-018-2147-5. Epub 2018 Dec 12. Surg Radiol Anat. 2019. PMID: 30542927 Free PMC article.
References
-
- Caffey J. Achondroplasia of pelvis and lumbo-sacral spine: Some roentgenographic features. AJR. 1958;80:449–57. - PubMed
-
- Kaufmann HJ. Rontgenbefunde am kindlichen becken bei angeborenen skelettaffektionen und chromosomalen aberrationen. Stuttgart, Germany: Thieme; 1964. - PubMed
-
- Kohler A, Zimmer EA. Borderlands of the normal and early pathologic in skeletal roentgenology. Case JT. 10th ed. New York: Grune and Stratton; 1956.
-
- Solomon L, Warwick DJ, Nayagam S. Apley's Concise System of Orthopaedics and Fractures. Third Edition. Boca Raton: CRC Press; 2005. p. 209. ePDF.
LinkOut - more resources
Full Text Sources
Other Literature Sources