

The influence of the Ebola outbreak on presumptive and active tuberculosis in Bombali District, Sierra Leone
- PMID: 28744432
- PMCID: PMC5515561
- DOI: 10.5588/pha.16.0093
The influence of the Ebola outbreak on presumptive and active tuberculosis in Bombali District, Sierra Leone
Abstract
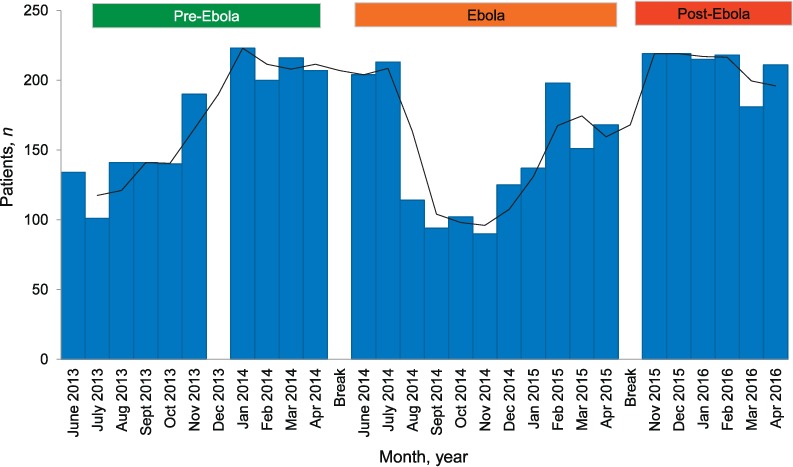
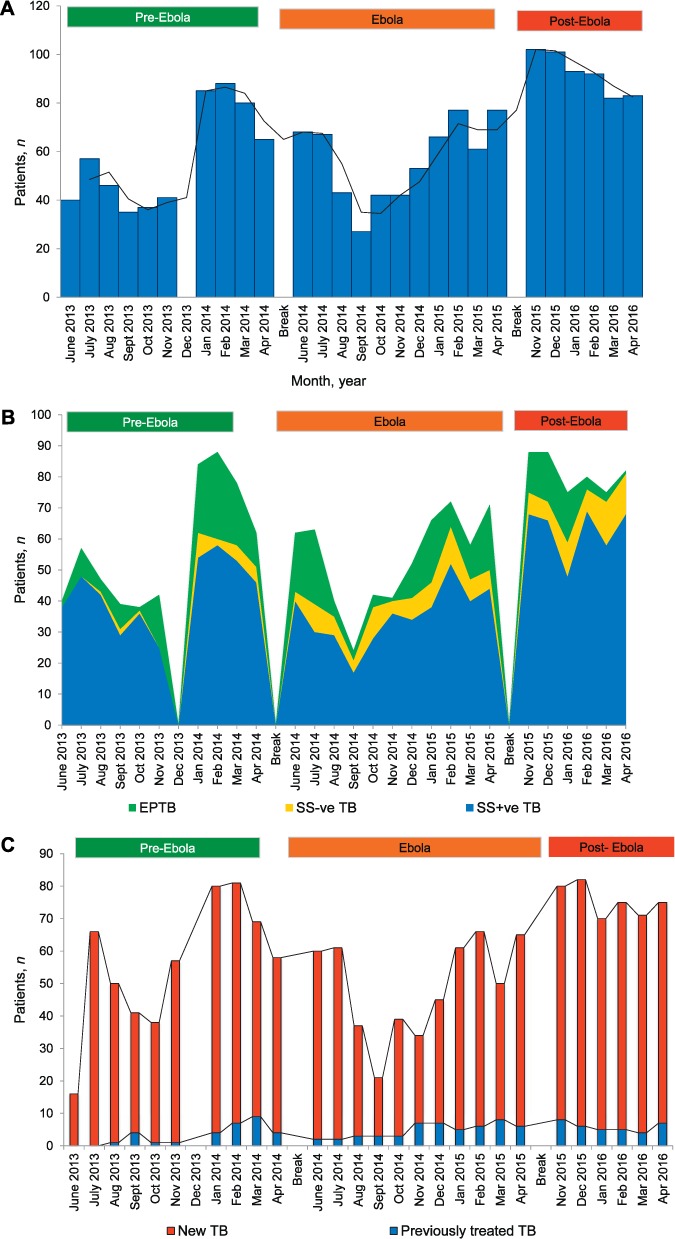
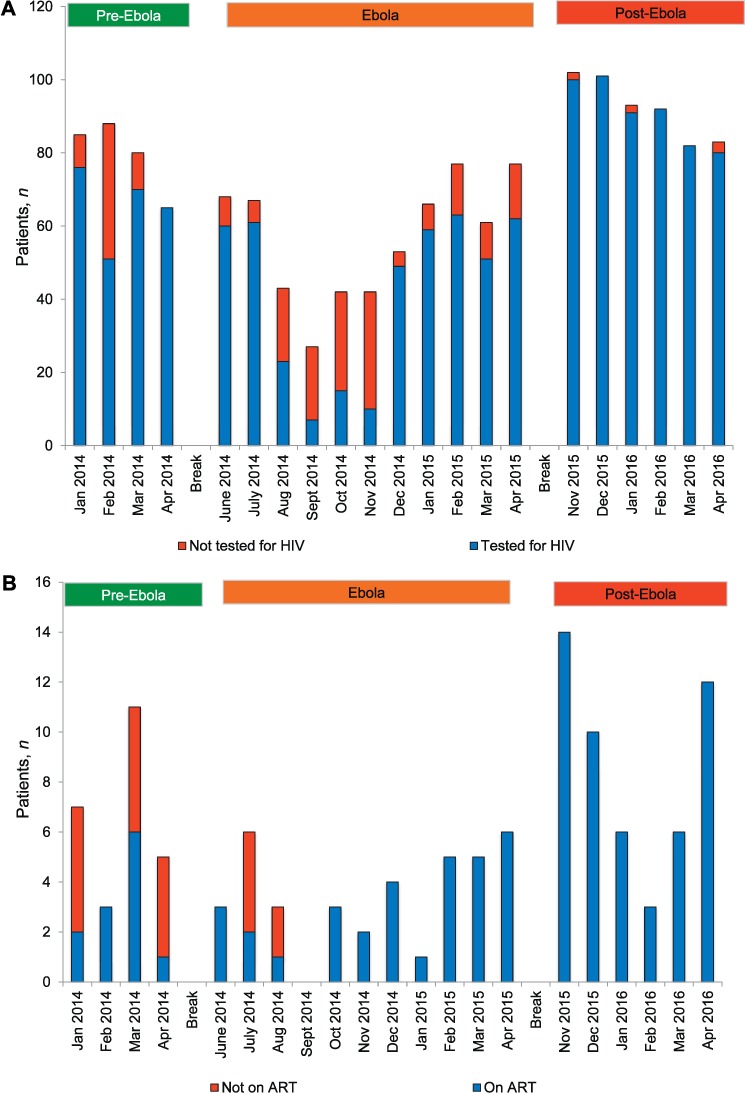
Setting: Bombali District, rural Sierra Leone. Objective: To compare the number of patients with presumptive tuberculosis (TB), the number of patients registered with TB (including testing for the human immunodeficiency virus [HIV] and initiation on antiretroviral therapy [ART]) and treatment outcomes during the pre-Ebola, Ebola and post-Ebola disease outbreak periods between 2013 and 2016. Design: This was a cross-sectional study and retrospective cohort analysis of treatment outcomes. Results: The mean monthly number of patients with presumptive TB before, during and post-Ebola was respectively 169, 145 and 210. The mean monthly number of registered TB cases was respectively 57, 57 and 96. Smear-positive TB was the most frequent type of TB, at 75%, 66% and 77%. The proportion of TB patients tested for HIV was 82% pre-Ebola, 74% Ebola and 99% post-Ebola. The proportion of HIV-positive patients with TB initiated on ART was respectively 46%, 85% and 100%. Treatment success among TB patients was 71% in the pre-Ebola period and 89% in the Ebola period (P < 0.001). Conclusion: During the Ebola outbreak, there were decreases in the number of presumptive TB patients and in the proportions of patients diagnosed with smear-positive TB and tested for HIV. The initiation of ART in HIV-infected TB patients and treatment outcomes remained acceptable. Pre-emptive actions are needed to maintain adequate control activities in future outbreaks.
Contexte : District de Bombali, Sierra Leone rurale.Objectif : Comparer le nombre de patients présumés tuberculeux (TB), le nombre enregistrés comme TB (incluant le test du virus de l'immunodéficience humaine [VIH] et la mise en route du traitement antirétroviral [TAR]) et les résultats du traitement pendant les périodes avant, pendant et après Ebola, entre 2013 et 2016.Schéma : Une étude transversale et analyse rétrospective de cohorte des résultats du traitement.Résultats : Le nombre moyen mensuel de patients présumés TB a été 169 avant Ebola, 145 pendant Ebola et 210 après Ebola. Le nombre mensuel moyen de cas de TB enregistrés a été 57 avant Ebola, 57 pendant Ebola et 96 après Ebola. La TB à frottis positif a été le type le plus fréquent, avec 75% avant Ebola, 66% pendant Ebola et 77% après Ebola. Les proportions de patients tuberculeux testés pour le VIH ont été 82% avant Ebola, 74% pendant Ebola et 99% après Ebola et pour les patients tuberculeux VIH positifs mis sous TAR, ces proportions ont été 46% avant Ebola, 85% pendant Ebola et 100% après Ebola. Le taux de succès du traitement des patients tuberculeux a été de 71% pendant les périodes avant Ebola et de 89% pendant Ebola (P < 0,001).Conclusion : Pendant la période de l'Ebola, il y a eu une diminution du nombre de patients présumés tuberculeux et dans les proportions de patients ayant eu un diagnostic de TB à frottis positif et un test VIH. La mise en route du TAR chez les patients infectés par le VIH et les résultats du traitement sont restés acceptables. Des actions préventives sont requises afin de maintenir des activités de lutte suffisantes lors de futures flambée épidémiques.
Marco de referencia: El distrito rural de Bombali en Sierra Leona.Objetivo: Comparar el número de pacientes con presunción clínica de tuberculosis (TB), el número de casos registrados de TB (con inclusión de las pruebas diagnósticas del virus de la inmunodeficiencia humana [VIH] y el inicio del tratamiento antirretrovírico [TAR]) y los desenlaces terapéuticos durante el período anterior a la epidemia del Ébola, durante la misma y después de ella del 2013 al 2016.Método: Un estudio transversal con un análisis retrospectivo de cohortes de los desenlaces terapéuticos.Resultados: El promedio mensual de pacientes con presunción clínica de TB fue como sigue: 169 antes de la epidemia del Ébola, 145 durante la epidemia y 210 después de la misma. El promedio mensual de casos registrados de TB fue 57 antes de la epidemia, 57 durante el brote y 96 después de la misma. La TB con baciloscopia positiva fue el tipo de enfermedad más frecuente y su proporción fue 75% antes de la epidemia del Ébola, 66% durante la misma y 77% después de ella. La proporción de pacientes TB que contaban con pruebas diagnósticas del VIH fue como sigue: 82% antes de la epidemia, 74% durante la misma y 99% después de ella y la proporción de pacientes con diagnóstico de TB y positivos frente al VIH que iniciaron el TAR fue 46% antes de la epidemia, 85% durante la misma y 100% después de ella. El éxito del tratamiento antituberculoso fue de 71% en el período anterior al brote de enfermedad del Ébola y de 89% en el período posterior al mismo (P < 0,001).Conclusión: Durante el período de la epidemia de enfermedad del Ébola se observó una disminución del número de casos con presunción clínica de TB, de la proporción de diagnósticos de TB con baciloscopia positiva y de la proporción de pacientes con pruebas diagnósticas del VIH. La iniciación del TAR en los pacientes coinfectados por el VIH y TB y los desenlaces terapéuticos conservaron proporciones aceptables. Se precisan intervenciones anticipativas, con el fin de mantener actividades de control adecuadas durante los brotes epidémicos en el futuro.
Keywords: HIV status; HIV testing; SORT IT; TB treatment outcomes; antiretroviral therapy; operational research.
Conflict of interest statement
Conflicts of interest: none declared.
Figures
References
-
- Baize S, Pannetier D, Oestereich L.. Emergence of Zaire Ebola virus disease in Guinea. N Engl J Med 2014; 15: 1418– 1425. - PubMed
-
- Gostin L O, Lucey D, Phelan A.. The Ebola epidemic: a global health emergency. JAMA 2014; 11: 1095– 1096. - PubMed
-
- World Health Organization. . Ebola situation report—6 January 2016. Geneva, Switzerland: WHO, 2016. http://apps.who.int/ebola/current-situation/ebola-situation-report-6-jan... Accessed March 2017.
-
- Boozary A S, Farmer P E, Jha A K.. The Ebola outbreak, fragile health systems, and quality as a cure. JAMA 2014; 18: 1859– 1860. - PubMed
-
- Ulrich C M. Ebola is causing moral distress among African healthcare workers. BMJ 2014; 349: g6672. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources