

Influence of Ebola on tuberculosis case finding and treatment outcomes in Liberia
- PMID: 28744441
- PMCID: PMC5515566
- DOI: 10.5588/pha.16.0097
Influence of Ebola on tuberculosis case finding and treatment outcomes in Liberia
Abstract
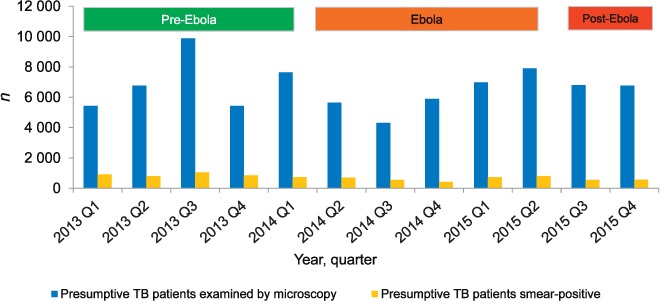
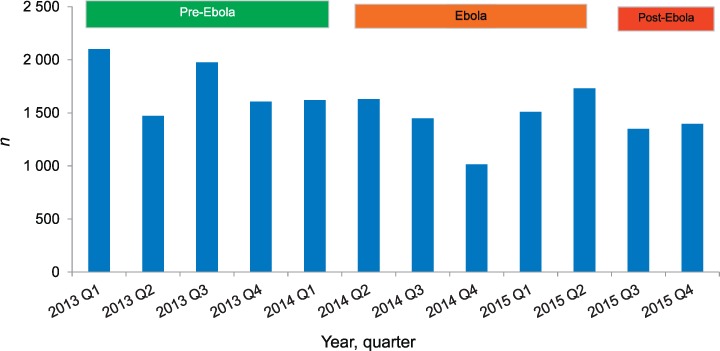
Setting: National Leprosy and Tuberculosis (TB) Control Programme, Liberia. Objectives: To assess TB case finding, including human immunodeficiency virus (HIV) associated interventions and treatment outcomes, before (January 2013-March 2014), during (April 2014-June 2015) and after (July-December 2015) the Ebola virus disease outbreak. Design: A cross-sectional study and retrospective cohort analysis of outcomes. Results: The mean quarterly numbers of individuals with presumptive TB and the proportion diagnosed as smear-positive were: pre-Ebola (n = 7032, 12%), Ebola (n = 6147, 10%) and post-Ebola (n = 6795, 8%). For all forms of TB, stratified by category and age group, there was a non-significant decrease in the number of cases from the pre-Ebola to the Ebola and post-Ebola periods. There were significant decreases in numbers of cases with smear-positive pulmonary TB (PTB) from the pre-Ebola period (n = 855), to the Ebola (n = 640, P < 0.001) and post-Ebola (n = 568, P < 0.001) periods. The proportions of patients tested for HIV, found to be HIV-positive and started on antiretroviral therapy decreased as follows: pre-Ebola (respectively 72%, 15% and 34%), Ebola (69%, 14% and 30%) and post-Ebola (68%, 12% and 26%). Treatment success rates among TB patients were: 80% pre-Ebola, 69% Ebola (P < 0.001) and 73% post-Ebola (P < 0.001). Loss to follow-up was the main contributing adverse outcome. Conclusion: The principal negative effects of Ebola were the significant decreases in diagnoses of smear-positive PTB, the declines in HIV testing and antiretroviral therapy uptake and poor treatment success. Ways to prevent these adverse effects from recurring in the event of another Ebola outbreak need to be found.
Contexte : Programme national de la tuberculose (TB), Liberia.Objectifs : Evaluer la détection des cas de TB, y compris les interventions associées au virus de l'immunodéficience humaine (VIH) et les résultats du traitement, avant (1 janvier 2013–31 mars 2014), pendant (1 avril 2014–30 juin 2015) et après la flambée d'Ebola (1 juillet–31 décembre 2015).Schéma : Une etude transversale et analyse de cohorte rétrospective des résultats.Résultats : Le nombre moyen mensuel par trimestre de présomptions de TB et de pourcentages de frottis positifs détectés était : pré-Ebola (n = 7032, 12%), pendant Ebola (n = 6147, 10%) et post-Ebola (n = 6795, 8%). Pour les TB toutes formes, stratifiées par catégorie et groupe d'âge, il y a eu une diminution non significative des nombres des périodes pré-Ebola à pendant Ebola et post-Ebola. Il y a eu une diminution significative des TB pulmonaire à frottis positif : pré-Ebola (855), pendant-Ebola (640, P < 0,001) et post-Ebola (568, P < 0,001). Les proportions de patients testés pour le VIH, trouvés VIH positifs et mis sous traitement antirétroviral (TAR) ont diminué : pré-Ebola (respectivement 72%, 15% et 34%), Ebola (69%, 14% et 30%) et post-Ebola (68%, 12% et 26%). Les taux de succès du traitement des patients TB ont été 80% pré-Ebola, 69% pendant Ebola (P < 0,001) et 73% post-Ebola (P < 0,001), avec les pertes de vue comme contributions principales aux résultats défavorables.Conclusion : Les principaux effets négatifs d'Ebola ont été des diminutions significatives du diagnostic de TBP à frottis positif, des déclins du test VIH et de la prise du TAR et un résultat médiocre du traitement. Il faut trouver des moyens d'éviter que ces effets négatifs ne surviennent à nouveau en cas de nouvelle épidémie.
Marco de referencia: El programa nacional contra la tuberculosis (TB) de Liberia.Objetivos: Evaluar la búsqueda de casos de TB teniendo en cuenta las intervenciones asociadas con el virus de la inmunodeficiencia humana (VIH) y examinar los desenlaces terapéuticos antes del brote epidémico de fiebre hemorrágica del Ébola (de 1 enero del 2013 a 31 marzo del 2014), durante el brote (del 1 abril del 2014 a 30 junio del 2015) y después del mismo (de 1 julio a 31 diciembre del 2015).Método: Un estudio transversal con análisis de cohortes retrospectivo de los desenlaces terapéuticos.Resultados: Antes de la epidemia, el promedio mensual por trimestres de los casos con presunción de TB fue 7032 (12% de baciloscopias positivas), durante el brote fue 6147 (10%) y después de la epidemia fue 6795 (8%). En todos los casos de TB, estratificados por categorías y grupos de edad, durante la epidemia y después de ella se observó una disminución no significativa de las cifras, en comparación con el período anterior a la epidemia. Ocurrió una neta disminución de los casos de TB pulmonar con baciloscopia positiva, a saber: antes de la epidemia del Ébola n = 855, durante el brote n = 640 (P < 0,001) y después del mismo n = 568 (P < 0,001). Se observó una disminución de la proporción de pacientes en quienes se practicó la prueba del VIH, que obtuvieron un resultado positivo y que iniciaron el tratamiento antirretrovírico (ART), respectivamente como sigue: antes del brote del Ébola 72%, 15% y 34%, durante la epidemia 69%, 14% y 30% y después del brote 68%, 12% y 26%. La tasa de éxito del tratamiento antituberculoso fue 80% antes del brote, 69% durante la epidemia (P < 0,001) y 7% después de la misma (P < 0,001); el desenlace desfavorable predominante fue la pérdida durante el seguimiento.Conclusión: Las principales consecuencias negativas de la epidemia del Ébola fueron una disminución considerable en el diagnóstico de TB pulmonar con baciloscopia positiva, una reducción de la práctica de la prueba del VIH y de la iniciación del ART y tasas insuficientes de éxito terapéutico. Se recomienda definir las medidas que puedan evitar estas consecuencias adversas, en la eventualidad de una futura epidemia.
Keywords: HIV testing; SORT IT; TB treatment outcomes; operational research; smear-positive pulmonary tuberculosis.
Conflict of interest statement
Conflicts of interest: none declared.
Figures



References
-
- World Health Organization. . Global tuberculosis report, 2015. WHO/HTM/TB/2015.22 Geneva, Switzerland: WHO, 2015.
-
- World Health Organization. . Treatment of tuberculosis. Guidelines. 4th ed WHO/HTM/TB/2009.420 Geneva, Switzerland: WHO, 2010. - PubMed
-
- World Health Organization. . Global tuberculosis report, 2014. WHO/HTM/TB/2014.08 Geneva, Switzerland: WHO, 2014.
-
- Baize S, Pannetier D, Oestreich L.. Emergence of Zaire Ebola virus disease in Guinea. N Engl J Med 2014; 15: 1418– 1425. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous