

Streptococcus intermedius: an unusual cause of spinal epidural abscess
- PMID: 28744508
- PMCID: PMC5506302
- DOI: 10.21037/jss.2017.05.04
Streptococcus intermedius: an unusual cause of spinal epidural abscess
Abstract
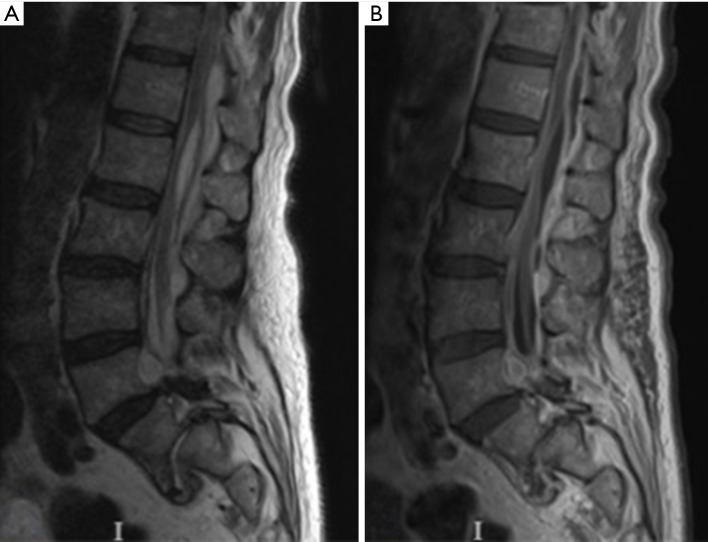
Spinal epidural abscess (SEA) following dental procedures is a rarely reported entity. Here, we present a unique case of a 74-year-old immunocompetent man who developed severe lower back pain and bilateral lower extremity weakness 4 days following two root canal procedures. Lumbar spine magnetic resonance imaging (MRI) showed several pockets of epidural abscesses extending from L1 through L5. Blood cultures grew Streptococcus intermedius, an anaerobic commensal bacterium of the normal flora of the mouth and upper airways. The patient was treated with IV penicillin for 7 days but his symptoms continued to deteriorate. A repeat MRI showed extension of the epidural abscess to T10-T11 level. The patient was emergently transferred to our hospital where he underwent bilateral decompressive laminectomy of T10 through S1 and abscess evacuation. Pus culture was positive for Streptococcus intermedius, which confirmed the diagnosis and the treatment plan. He was discharged on intravenous (IV) penicillin for 6 weeks. His symptoms improved significantly postoperatively as he retained his baseline strength in his lower extremity.
Keywords: Streptococcus intermedius; root canal; spinal epidural abscess (SEA); tooth extraction.
Conflict of interest statement
Conflicts of Interest: Ali Bydon is a recipient of a research grant from DePuy Spine, and serves on the clinical advisory board of MedImmune, LLC.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials