

Clinical outcomes of medial collateral ligament injury in total knee arthroplasty
- PMID: 28746219
- PMCID: PMC5627845
- DOI: 10.1097/MD.0000000000007617
Clinical outcomes of medial collateral ligament injury in total knee arthroplasty
Abstract
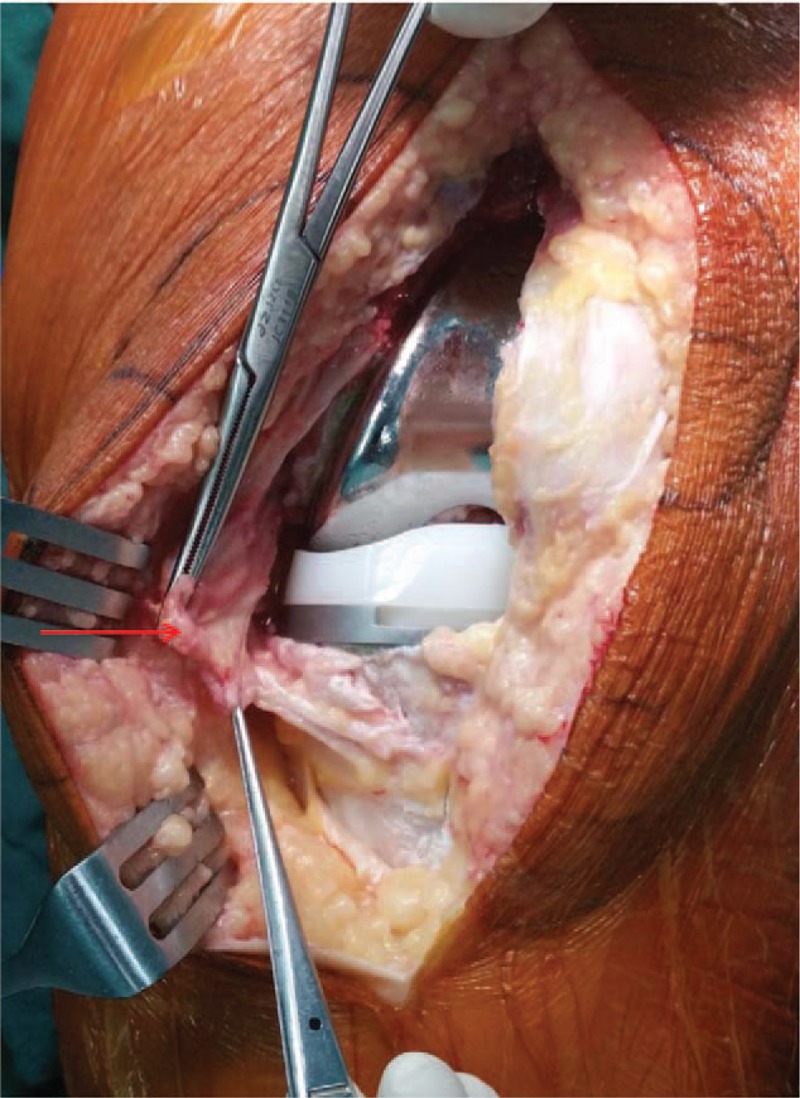
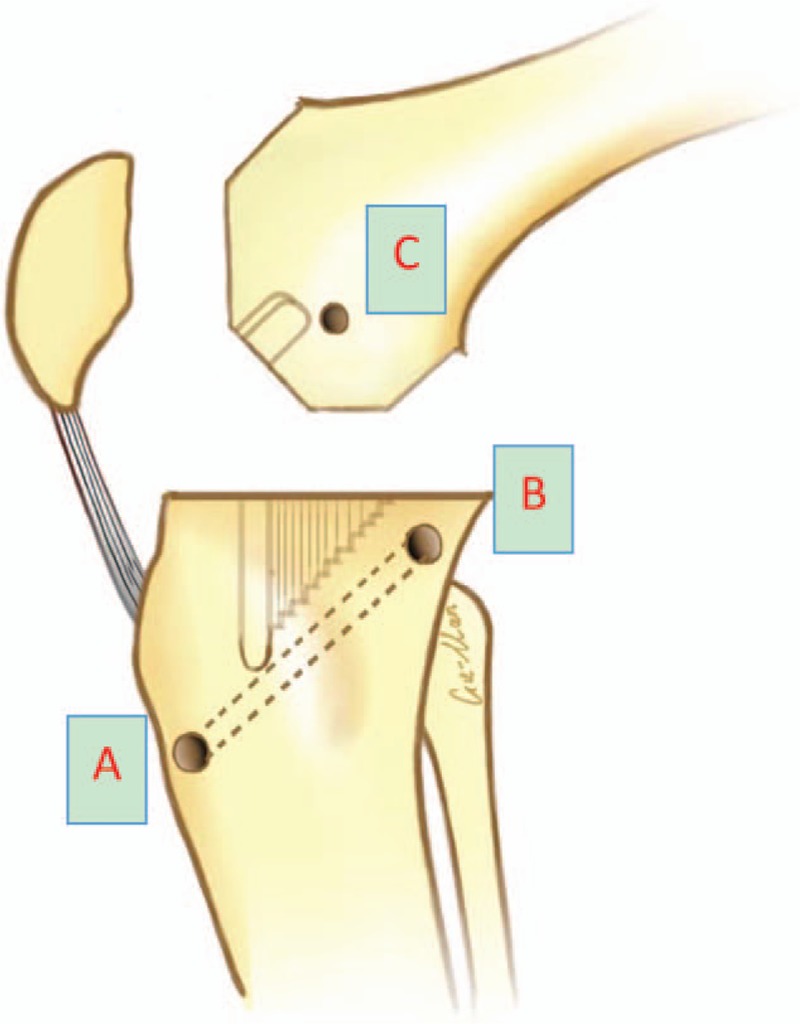
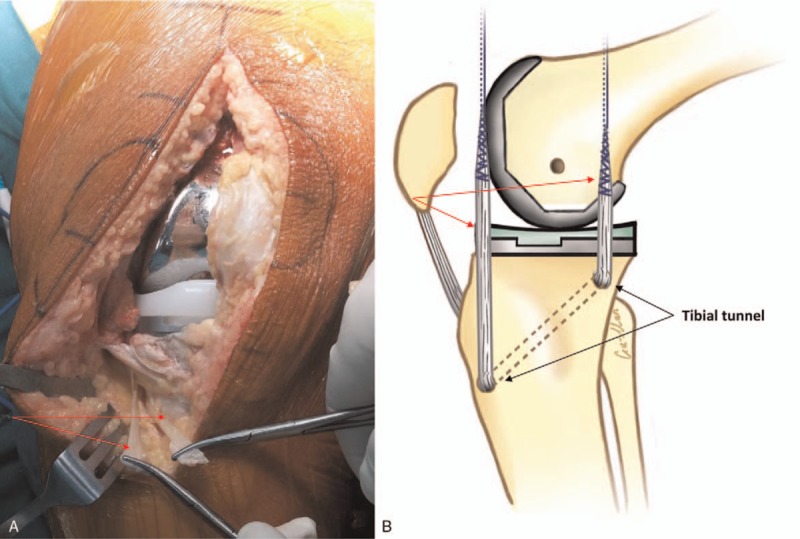
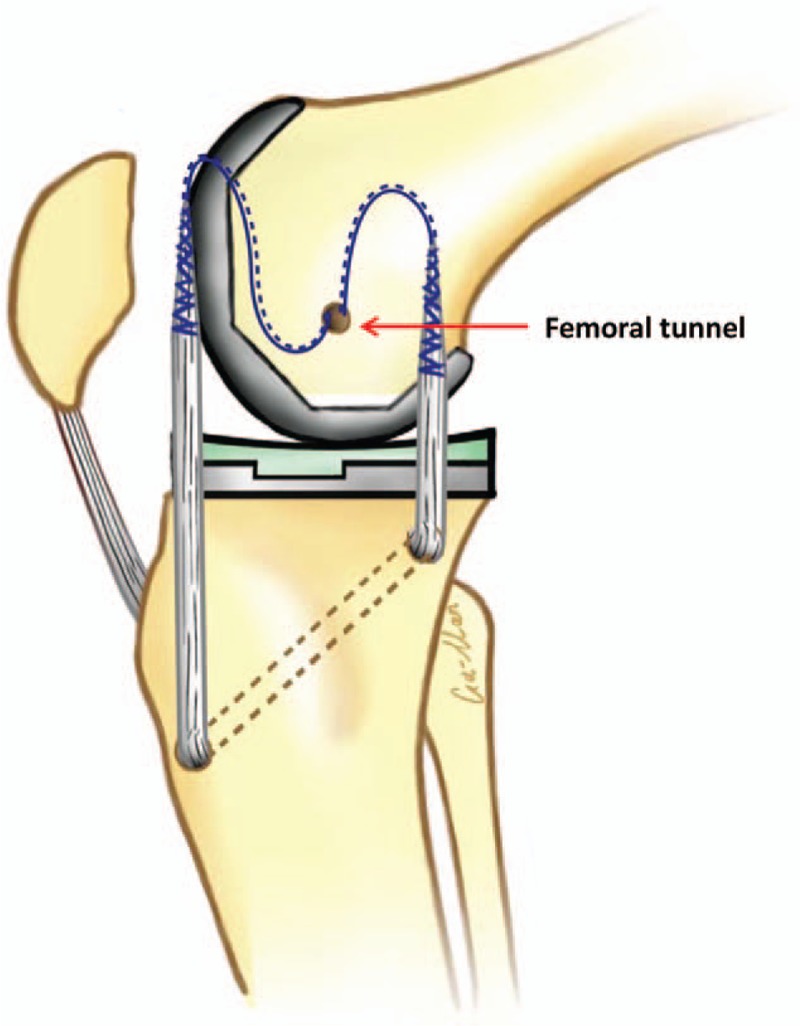
Intraoperative injury to the medial collateral ligament (MCL) during total knee arthroplasty (TKA) is a rare but severe complication. The main treatment methods are primary repair and revision with a more constrained implant; however, the clinical outcomes of primary reconstruction without a constrained implant have rarely been reported.A retrospective study was performed to evaluate the prevalence of iatrogenic injury to the MCL during primary TKA, and to report the clinical outcomes of MCL reconstruction without the use of a constrained device.A total of 1749 patients (2054 knees) underwent primary TKA between 2007 and 2013 and were retrospectively evaluated. Seventeen patients (0.83%) experienced an MCL injury intraoperatively, and the remaining 1732 patients (2037 knees) were considered as the controls. We attempted to reconstruct the MCL with an unconstrained prosthesis in all patients. The Knee Society Score (KSS) was used to evaluate knee function after an average 51-month follow-up (range, 36-72 months).No patients were lost during the follow-up period. In the MCL injury group, the mean KSS was 84.7 for function and 87.7 for pain, while the scores were 87.9 and 90.6, respectively, in the control group. No patient treated with MCL reconstruction without increased prosthetic constraint experienced knee instability requiring revision.MCL reconstruction without a constrained implant achieved excellent results for MCL injury during TKA.
Level of evidence: Level IV, therapeutic study.
Figures
References
-
- Leopold SS, McStay C, Klafeta K, et al. Primary repair of intraoperative disruption of the medical collateral ligament during total knee arthroplasty. J Bone Joint Surg Am 2001;83:86–91. - PubMed
-
- Siqueira MB, Haller K, Mulder A, et al. Outcomes of medial collateral ligament injuries during total knee arthroplasty. J Knee Surg 2016; 29:68–73. - PubMed
-
- Cameron HU, Hunter GA. Failure in total knee arthroplasty. Mechanisms, revisions, and results. Clin Orthop Relat Res 1982;170:141. - PubMed
-
- Giori NJ, Lewallen DG. Total knee arthroplasty in limbs affected by poliomyelitis. J Bone Joint Surg Am 2002;84:1157. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
