

Clinical Significance of Four Molecular Subtypes of Gastric Cancer Identified by The Cancer Genome Atlas Project
- PMID: 28747339
- PMCID: PMC5785562
- DOI: 10.1158/1078-0432.CCR-16-2211
Clinical Significance of Four Molecular Subtypes of Gastric Cancer Identified by The Cancer Genome Atlas Project
Abstract
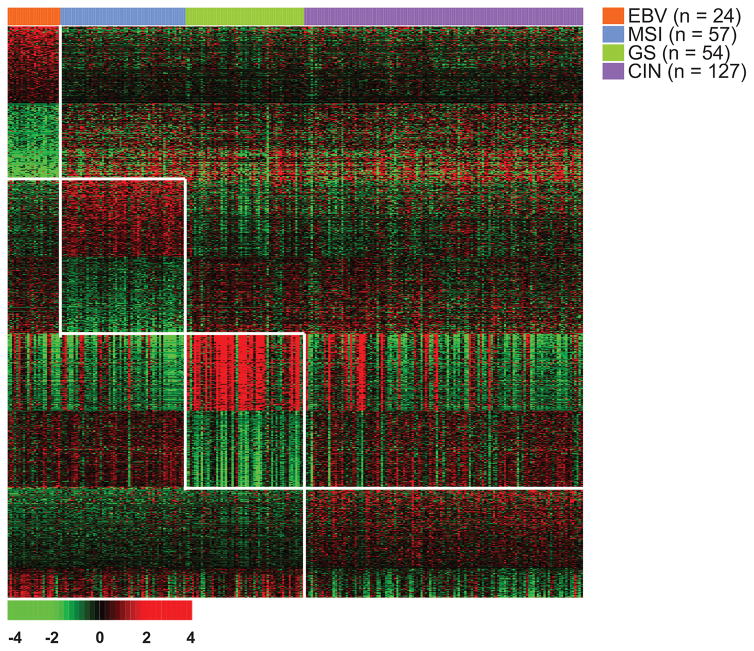
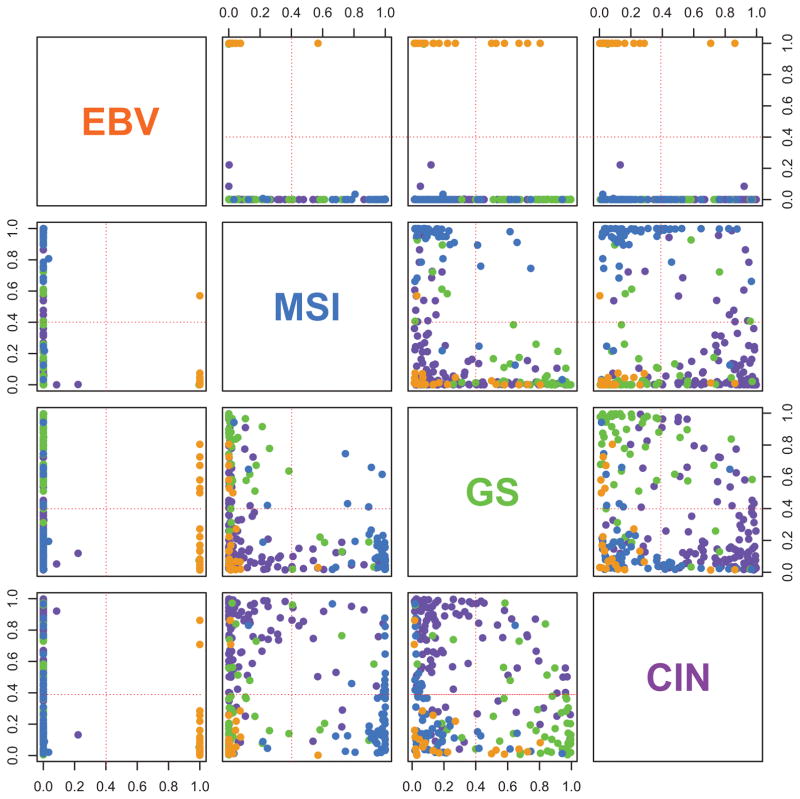
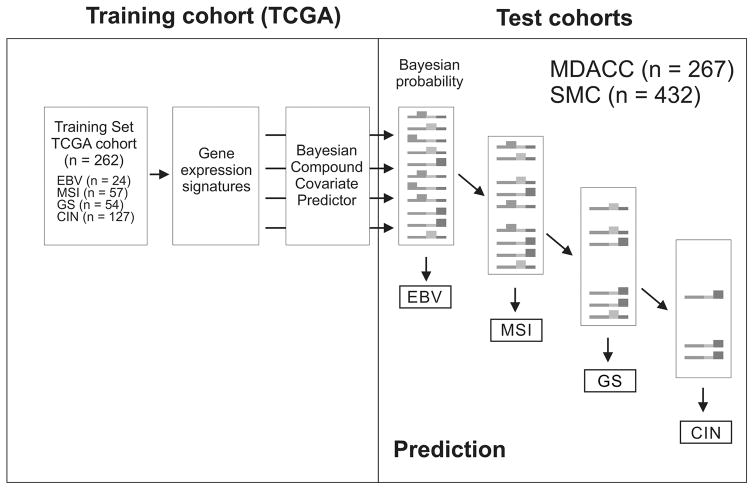
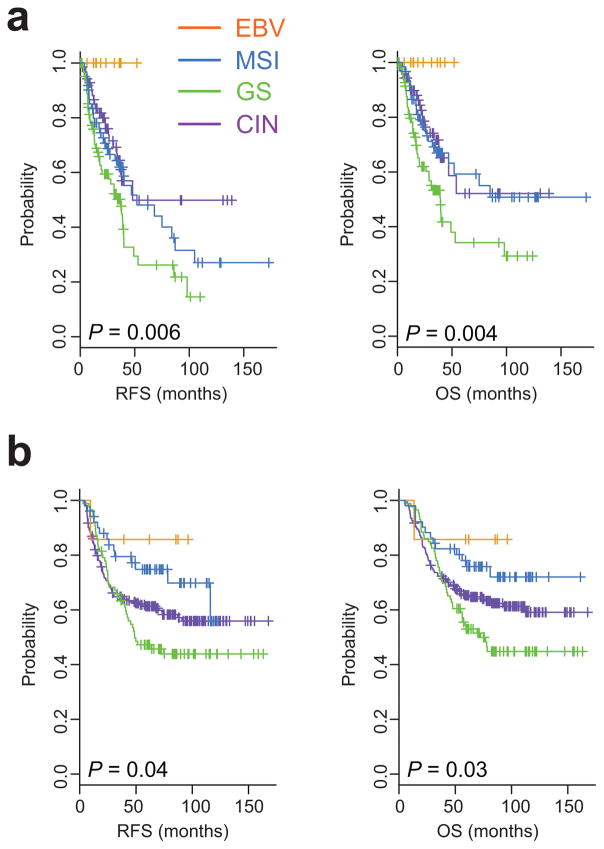
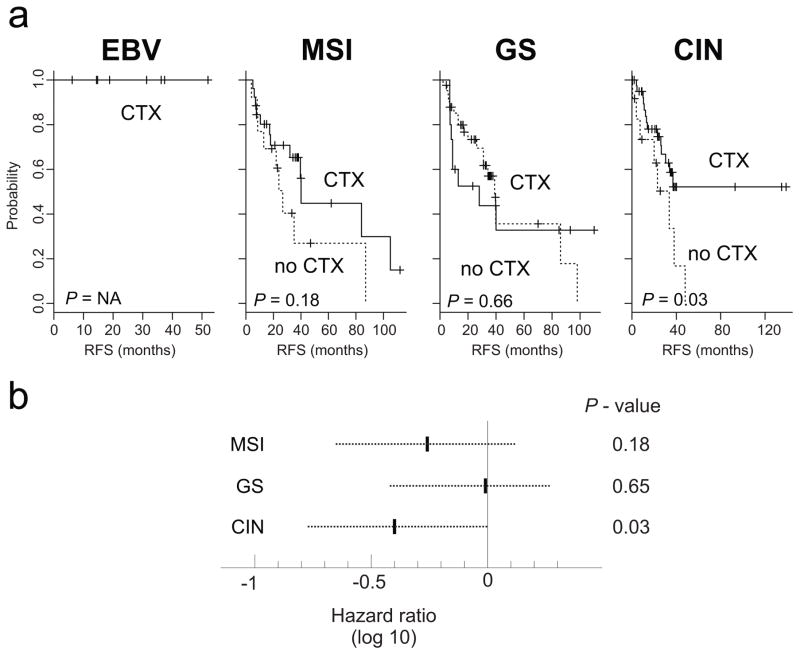
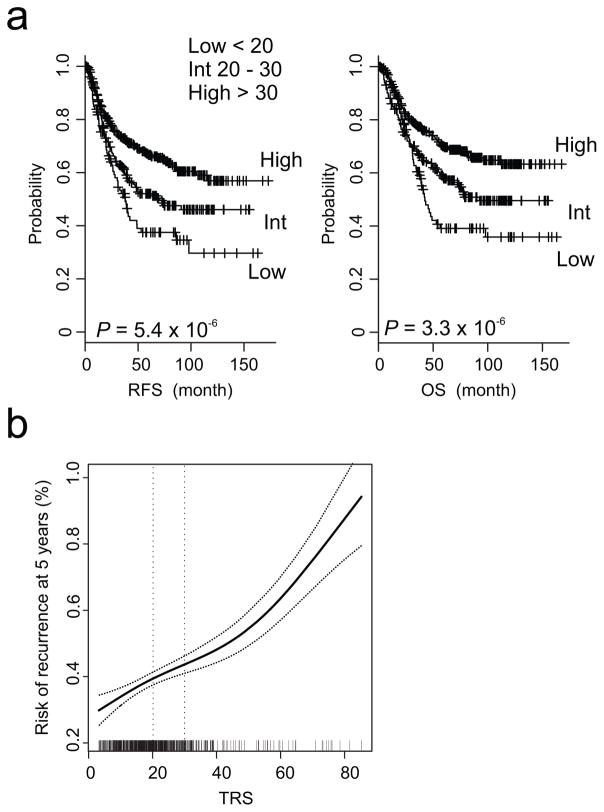
Purpose: The Cancer Genome Atlas (TCGA) project recently uncovered four molecular subtypes of gastric cancer: Epstein-Barr virus (EBV), microsatellite instability (MSI), genomically stable (GS), and chromosomal instability (CIN). However, their clinical significances are currently unknown. We aimed to investigate the relationship between subtypes and prognosis of patients with gastric cancer.Experimental Design: Gene expression data from a TCGA cohort (n = 262) were used to develop a subtype prediction model, and the association of each subtype with survival and benefit from adjuvant chemotherapy was tested in 2 other cohorts (n = 267 and 432). An integrated risk assessment model (TCGA risk score) was also developed.Results: EBV subtype was associated with the best prognosis, and GS subtype was associated with the worst prognosis. Patients with MSI and CIN subtypes had poorer overall survival than those with EBV subtype but better overall survival than those with GS subtype (P = 0.004 and 0.03 in two cohorts, respectively). In multivariate Cox regression analyses, TCGA risk score was an independent prognostic factor [HR, 1.5; 95% confidence interval (CI), 1.2-1.9; P = 0.001]. Patients with the CIN subtype experienced the greatest benefit from adjuvant chemotherapy (HR, 0.39; 95% CI, 0.16-0.94; P = 0.03) and those with the GS subtype had the least benefit from adjuvant chemotherapy (HR, 0.83; 95% CI, 0.36-1.89; P = 0.65).Conclusions: Our prediction model successfully stratified patients by survival and adjuvant chemotherapy outcomes. Further development of the prediction model is warranted. Clin Cancer Res; 23(15); 4441-9. ©2017 AACR.
©2017 American Association for Cancer Research.
Conflict of interest statement
No potential conflicts of interest were disclosed.
Figures
References
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. - PubMed
-
- Bang YJ, Kim YW, Yang HK, Chung HC, Park YK, Lee KH, et al. Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): a phase 3 open-label, randomised controlled trial. Lancet. 2012;379(9813):315–21. - PubMed
-
- Cunningham D, Allum WH, Stenning SP, Thompson JN, van de Velde CJ, Nicolson M, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355(1):11–20. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
