

Brain hemorrhage recurrence, small vessel disease type, and cerebral microbleeds: A meta-analysis
- PMID: 28747441
- PMCID: PMC5580863
- DOI: 10.1212/WNL.0000000000004259
Brain hemorrhage recurrence, small vessel disease type, and cerebral microbleeds: A meta-analysis
Abstract
Objective: We evaluated recurrent intracerebral hemorrhage (ICH) risk in ICH survivors, stratified by the presence, distribution, and number of cerebral microbleeds (CMBs) on MRI (i.e., the presumed causal underlying small vessel disease and its severity).
Methods: This was a meta-analysis of prospective cohorts following ICH, with blood-sensitive brain MRI soon after ICH. We estimated annualized recurrent symptomatic ICH rates for each study and compared pooled odds ratios (ORs) of recurrent ICH by CMB presence/absence and presumed etiology based on CMB distribution (strictly lobar CMBs related to probable or possible cerebral amyloid angiopathy [CAA] vs non-CAA) and burden (1, 2-4, 5-10, and >10 CMBs), using random effects models.
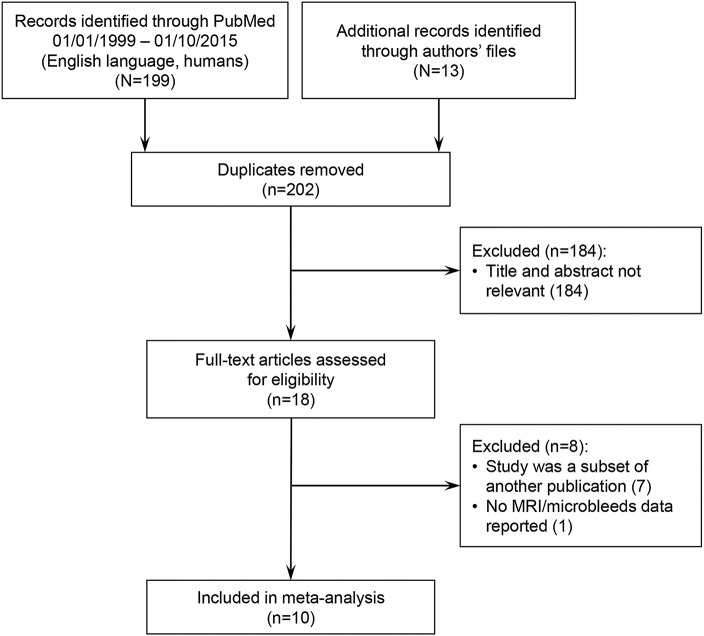
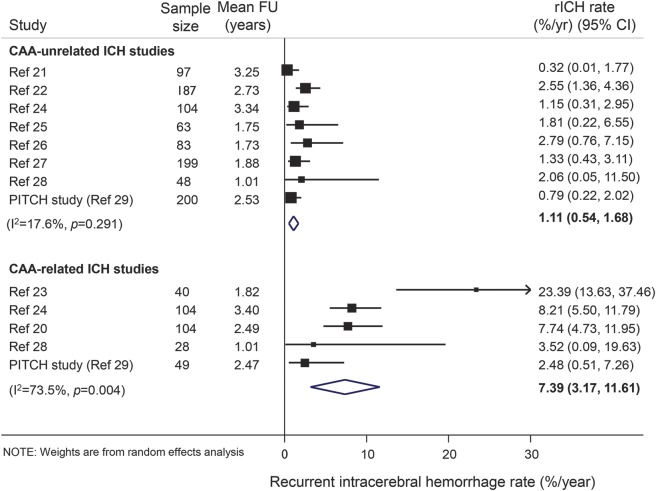
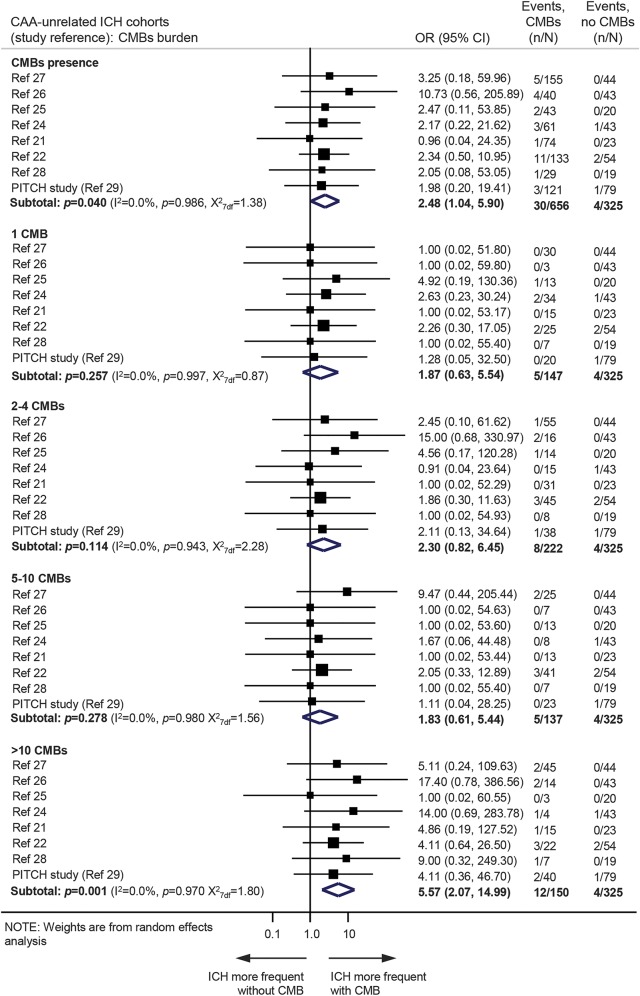
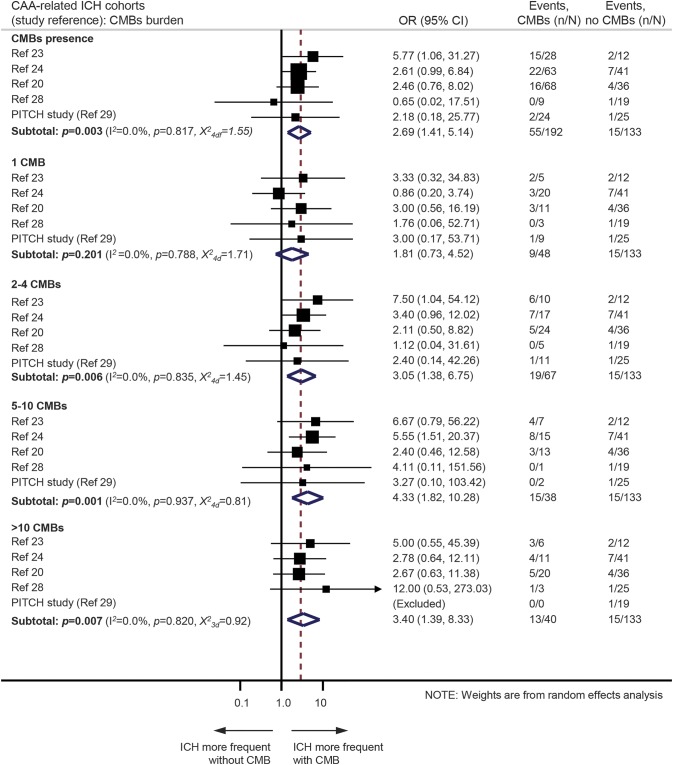
Results: We pooled data from 10 studies including 1,306 patients: 325 with CAA-related and 981 CAA-unrelated ICH. The annual recurrent ICH risk was higher in CAA-related ICH vs CAA-unrelated ICH (7.4%, 95% confidence interval [CI] 3.2-12.6 vs 1.1%, 95% CI 0.5-1.7 per year, respectively; p = 0.01). In CAA-related ICH, multiple baseline CMBs (versus none) were associated with ICH recurrence during follow-up (range 1-3 years): OR 3.1 (95% CI 1.4-6.8; p = 0.006), 4.3 (95% CI 1.8-10.3; p = 0.001), and 3.4 (95% CI 1.4-8.3; p = 0.007) for 2-4, 5-10, and >10 CMBs, respectively. In CAA-unrelated ICH, only >10 CMBs (versus none) were associated with recurrent ICH (OR 5.6, 95% CI 2.1-15; p = 0.001). The presence of 1 CMB (versus none) was not associated with recurrent ICH in CAA-related or CAA-unrelated cohorts.
Conclusions: CMB burden and distribution on MRI identify subgroups of ICH survivors with higher ICH recurrence risk, which may help to predict ICH prognosis with relevance for clinical practice and treatment trials.
Copyright © 2017 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Poon MT, Fonville AF, Al-Shahi Salman R. Long-term prognosis after intracerebral haemorrhage: systematic review and meta-analysis. J Neurol Neurosurg Psychiatry 2014;85:660–667. - PubMed
-
- Pantoni L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol 2010;9:689–701. - PubMed
-
- Charidimou A, Gang Q, Werring DJ. Sporadic cerebral amyloid angiopathy revisited: recent insights into pathophysiology and clinical spectrum. J Neurol Neurosurg Psychiatry 2012;83:124–137. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical