

Epidemiology, pathophysiology, and management of uric acid urolithiasis: A narrative review
- PMID: 28748117
- PMCID: PMC5512151
- DOI: 10.1016/j.jare.2017.04.005
Epidemiology, pathophysiology, and management of uric acid urolithiasis: A narrative review
Abstract
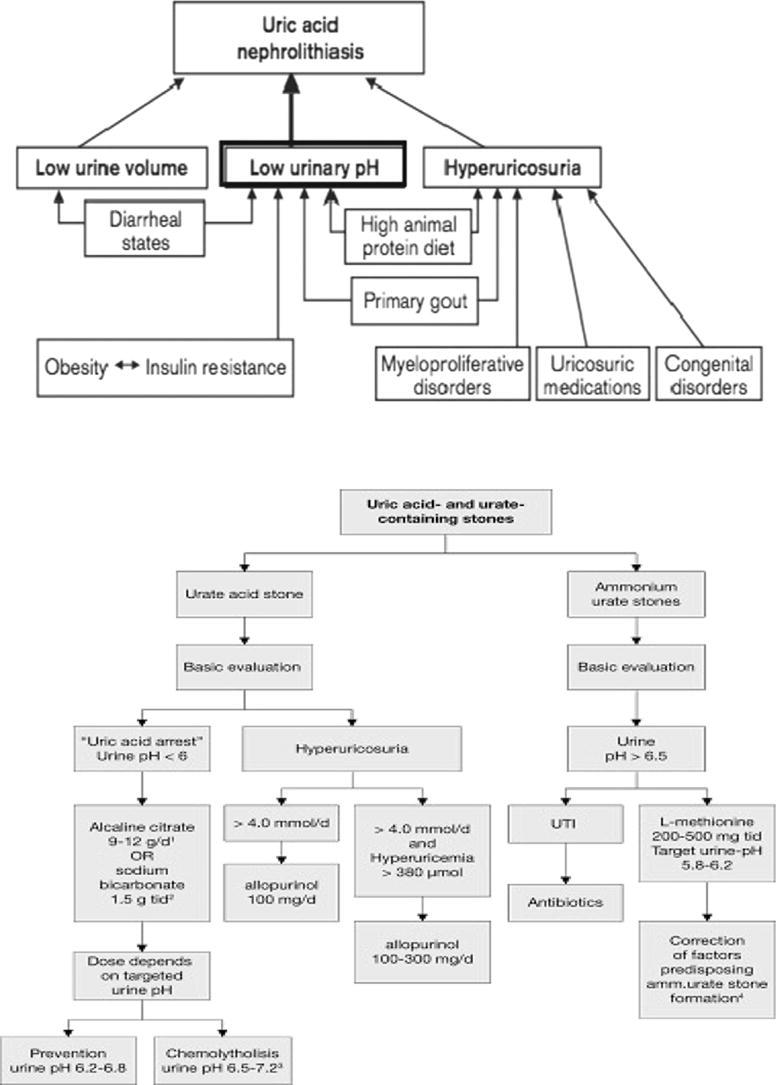
An in-depth comprehension of the epidemiology as well as pathophysiology of uric acid urolithiasis is important for the identification, treatment, and prophylaxis of calculi in these patients. Persistently low urinary pH, hyperuricosuria, and low urinary volume are the most important factors in pathogenesis of uric acid urolithiasis. Other various causes of calculus formation comprises of chronic diarrhea, renal hyperuricosuria, insulin resistance, primary gout, extra purine in the diet, neoplastic syndromes, and congenital hyperuricemia. Non-contrast-enhanced computed tomography is the radiologic modality of choice for early assessment of patients with renal colic. Excluding situations where there is acute obstruction, rising blood chemistry, severe infection, or unresolved pain, the initial management ought to be medical dissolution by oral chemolysis since this method has proved to be effective in most of the cases.
Keywords: Calculi; Chemolysis; Nephrolithiasis; Uric acid; Uric acid stones; Urinary stones; Urolithiasis; pH dissolution.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
