

CMR fluoroscopy right heart catheterization for cardiac output and pulmonary vascular resistance: results in 102 patients
- PMID: 28750642
- PMCID: PMC5530573
- DOI: 10.1186/s12968-017-0366-2
CMR fluoroscopy right heart catheterization for cardiac output and pulmonary vascular resistance: results in 102 patients
Abstract
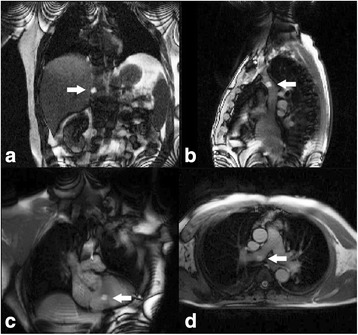
Background: Quantification of cardiac output and pulmonary vascular resistance (PVR) are critical components of invasive hemodynamic assessment, and can be measured concurrently with pressures using phase contrast CMR flow during real-time CMR guided cardiac catheterization.
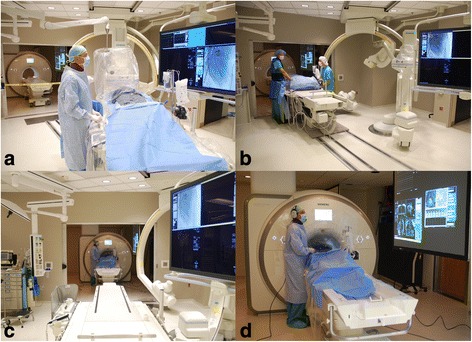
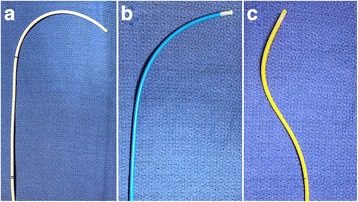
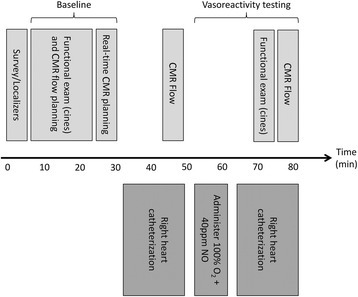
Methods: One hundred two consecutive patients underwent CMR fluoroscopy guided right heart catheterization (RHC) with simultaneous measurement of pressure, cardiac output and pulmonary vascular resistance using CMR flow and the Fick principle for comparison. Procedural success, catheterization time and adverse events were prospectively collected.
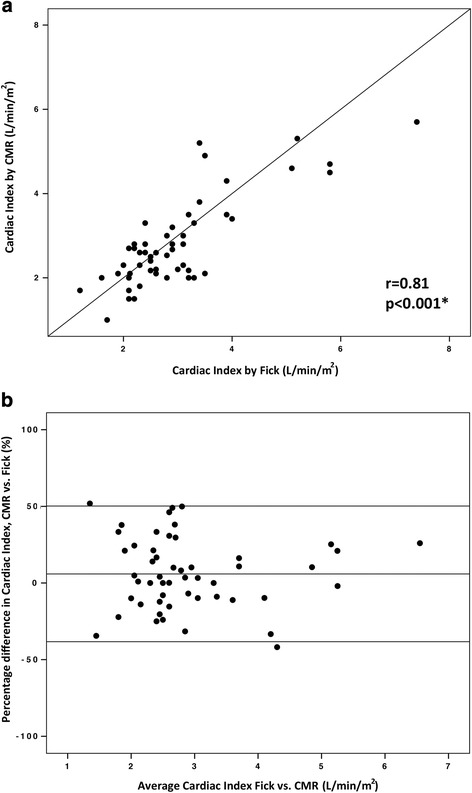
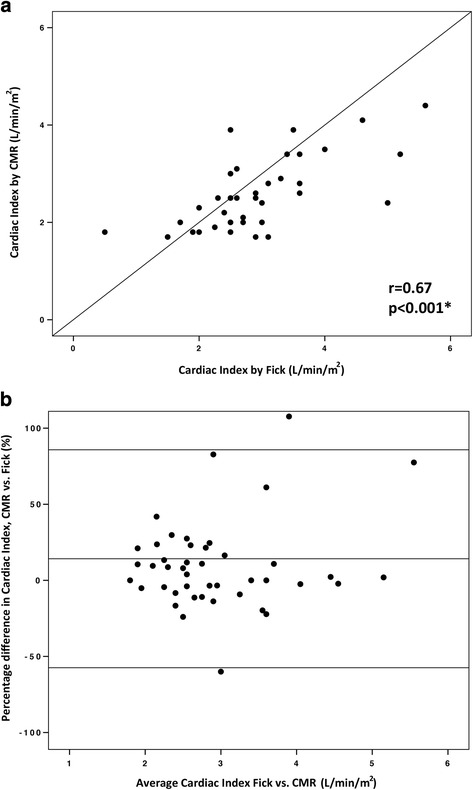
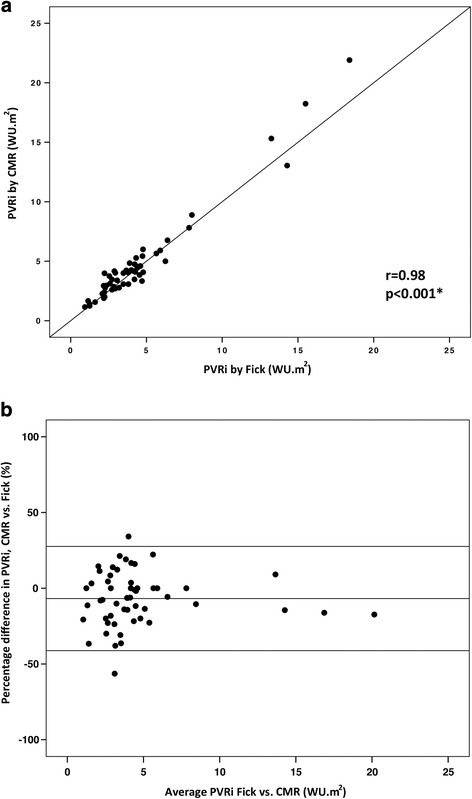
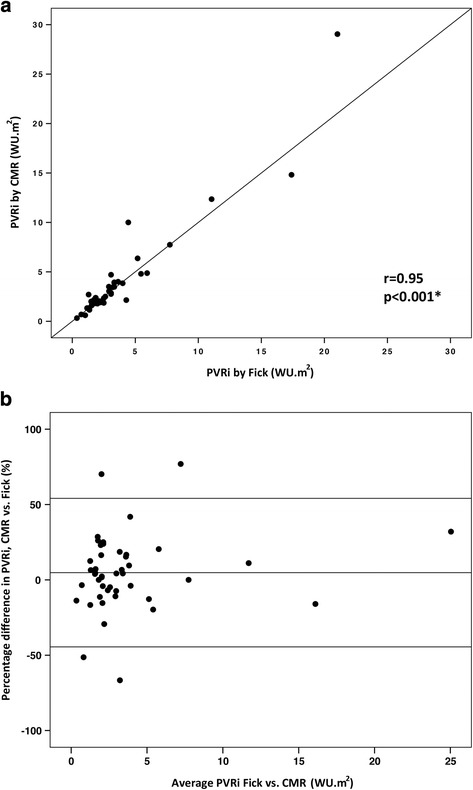
Results: RHC was successfully completed in 97/102 (95.1%) patients without complication. Catheterization time was 20 ± 11 min. In patients with and without pulmonary hypertension, baseline mean pulmonary artery pressure was 39 ± 12 mmHg vs. 18 ± 4 mmHg (p < 0.001), right ventricular (RV) end diastolic volume was 104 ± 64 vs. 74 ± 24 (p = 0.02), and RV end-systolic volume was 49 ± 30 vs. 31 ± 13 (p = 0.004) respectively. 103 paired cardiac output and 99 paired PVR calculations across multiple conditions were analyzed. At baseline, the bias between cardiac output by CMR and Fick was 5.9% with limits of agreement -38.3% and 50.2% with r = 0.81 (p < 0.001). The bias between PVR by CMR and Fick was -0.02 WU.m2 with limits of agreement -2.6 and 2.5 WU.m2 with r = 0.98 (p < 0.001). Correlation coefficients were lower and limits of agreement wider during physiological provocation with inhaled 100% oxygen and 40 ppm nitric oxide.
Conclusions: CMR fluoroscopy guided cardiac catheterization is safe, with acceptable procedure times and high procedural success rate. Cardiac output and PVR measurements using CMR flow correlated well with the Fick at baseline and are likely more accurate during physiological provocation with supplemental high-concentration inhaled oxygen.
Trial registration: Clinicaltrials.gov NCT01287026 , registered January 25, 2011.
Keywords: CMR; Cardiac MRI; Interventional MRI catheterization; Invasive hemodynamics; Phase contrast MRI flow; Real-time MRI; Right heart catheterization.
Conflict of interest statement
Authors’ information
Not applicable.
Ethics approval and consent to participate
The study was approved by the NHLBI Institutional Review Board and conducted under NHLBI Federalwide Assurance number FWA00000004. All subjects provided written informed consent.
Consent for publication
The protocol and NHLBI IRB approval include permission to use de-identified subject images in scientific communications.
Competing interests
NIH and Siemens Medical Systems have a collaborative research and development agreement for interventional CMR.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Winniford MD, Kern MJ, Lambert CR. Blood flow measurement and quantification of vascular stenoses. In: Pepine CJ, Hill JA, Lambert CR, editors. Diagnostic and therapeutic cardiac catheterization 3/e. Baltimore: Williams & Wilkins; 1998. pp. 399–441.
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
