

Factor H autoantibody is associated with atypical hemolytic uremic syndrome in children in the United Kingdom and Ireland
- PMID: 28750931
- PMCID: PMC5652378
- DOI: 10.1016/j.kint.2017.04.028
Factor H autoantibody is associated with atypical hemolytic uremic syndrome in children in the United Kingdom and Ireland
Abstract
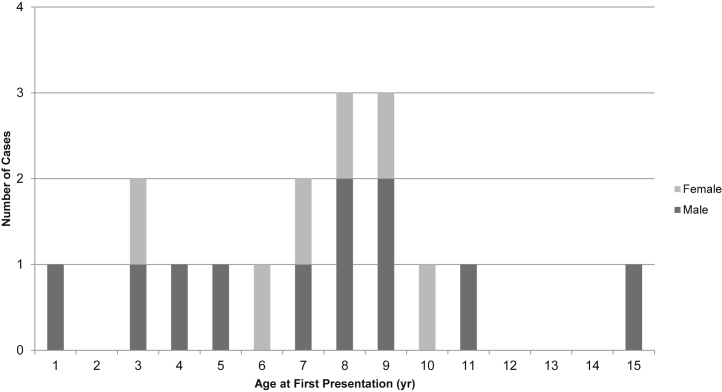
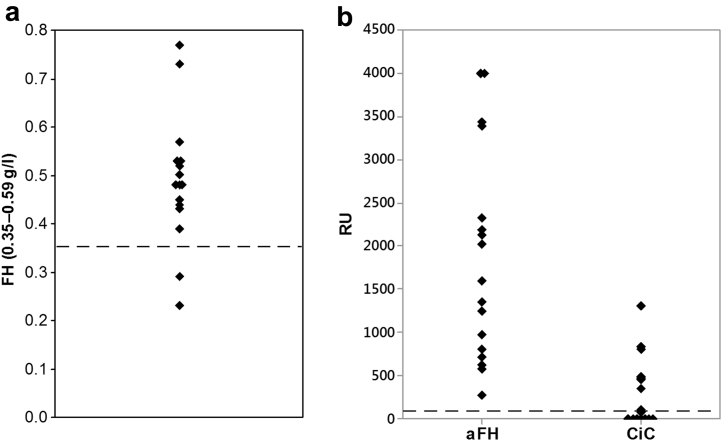
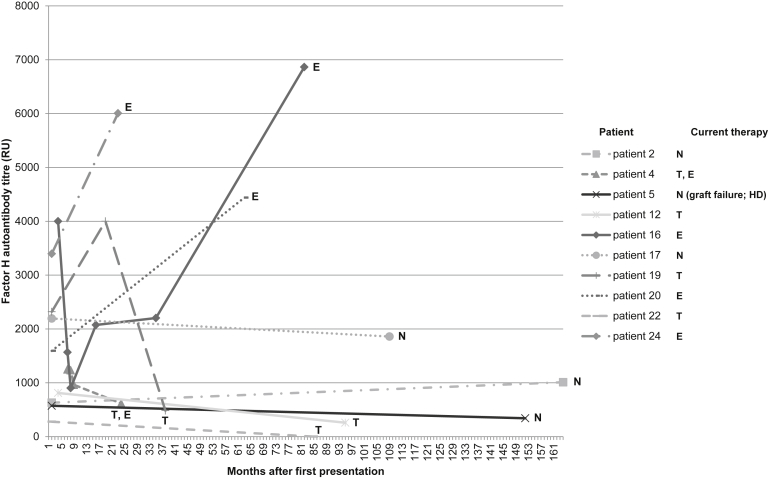
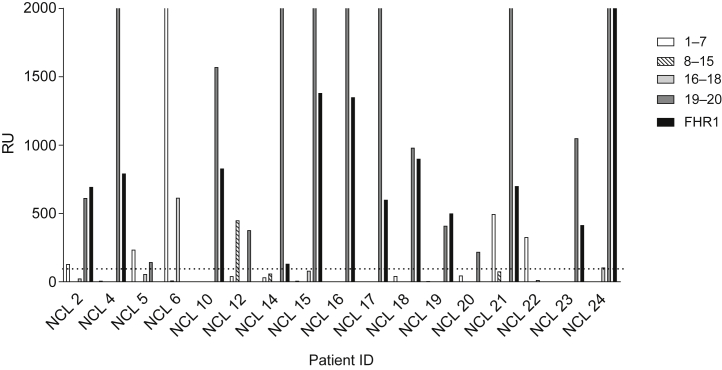
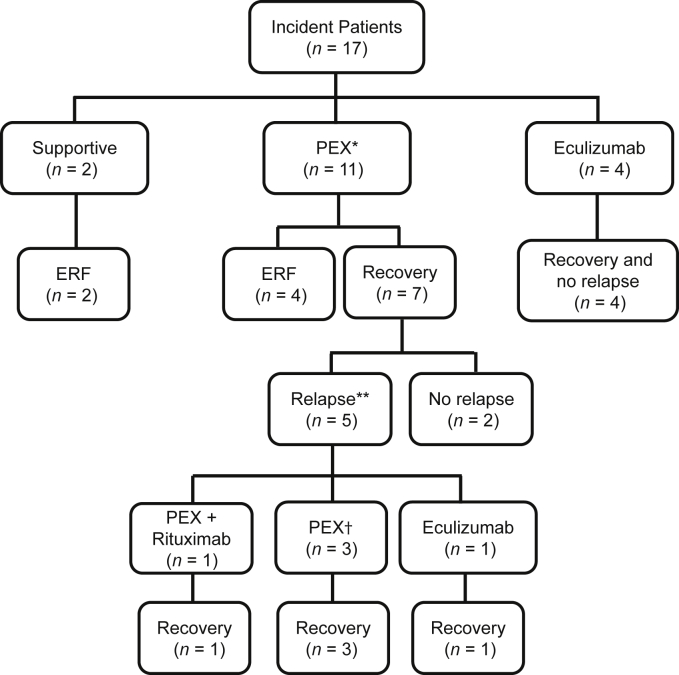
Factor H autoantibodies can impair complement regulation, resulting in atypical hemolytic uremic syndrome, predominantly in childhood. There are no trials investigating treatment, and clinical practice is only informed by retrospective cohort analysis. Here we examined 175 children presenting with atypical hemolytic uremic syndrome in the United Kingdom and Ireland for factor H autoantibodies that included 17 children with titers above the international standard. Of the 17, seven had a concomitant rare genetic variant in a gene encoding a complement pathway component or regulator. Two children received supportive treatment; both developed established renal failure. Plasma exchange was associated with a poor rate of renal recovery in seven of 11 treated. Six patients treated with eculizumab recovered renal function. Contrary to global practice, immunosuppressive therapy to prevent relapse in plasma exchange-treated patients was not adopted due to concerns over treatment-associated complications. Without immunosuppression, the relapse rate was high (five of seven). However, reintroduction of treatment resulted in recovery of renal function. All patients treated with eculizumab achieved sustained remission. Five patients received renal transplants without specific factor H autoantibody-targeted treatment with recurrence in one who also had a functionally significant CFI mutation. Thus, our current practice is to initiate eculizumab therapy for treatment of factor H autoantibody-mediated atypical hemolytic uremic syndrome rather than plasma exchange with or without immunosuppression. Based on this retrospective analysis we see no suggestion of inferior treatment, albeit the strength of our conclusions is limited by the small sample size.
Keywords: acute kidney injury; atypical hemolytic uremic syndrome; complement; factor H autoantibodies; thrombotic microangiopathy.
Copyright © 2017 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Sheerin N.S., Kavanagh D., Goodship T.H. A national specialized service in England for atypical haemolytic uraemic syndrome-the first year's experience. QJM. 2016;109:27–33. - PubMed
-
- Dragon-Durey M.A., Loirat C., Cloarec S. Anti-factor H autoantibodies associated with atypical hemolytic uremic syndrome. J Am Soc Nephrol. 2005;16:555–563. - PubMed
-
- Durey M.D., Sinha A., Togarsimalemath S.K. Anti-complement-factor H-associated glomerulopathies. Nat Rev Nephrol. 2016 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
