

ANMCO/SIC Consensus Document: cardiology networks for outpatient heart failure care
- PMID: 28751837
- PMCID: PMC5520754
- DOI: 10.1093/eurheartj/sux009
ANMCO/SIC Consensus Document: cardiology networks for outpatient heart failure care
Abstract
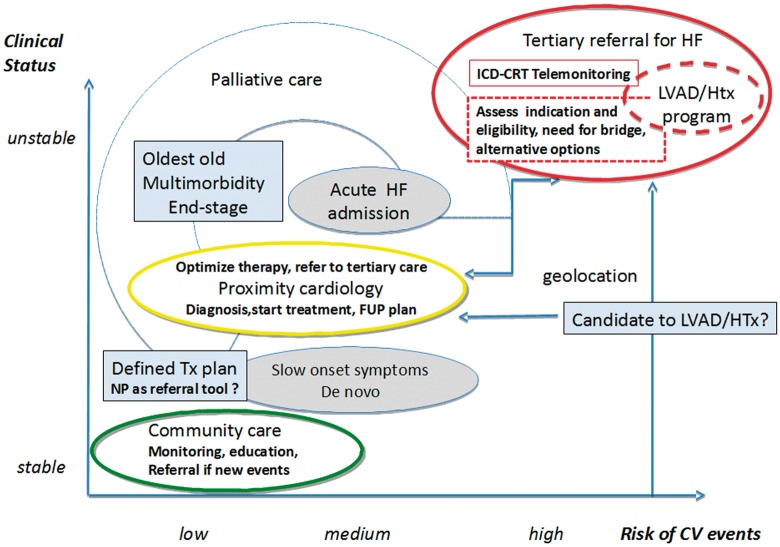
Changing demographics and an increasing burden of multiple chronic comorbidities in Western countries dictate refocusing of heart failure (HF) services from acute in-hospital care to better support the long inter-critical out-of- hospital phases of HF. In Italy, as well as in other countries, needs of the HF population are not adequately addressed by current HF outpatient services, as documented by differences in age, gender, comorbidities and recommended therapies between patients discharged for acute hospitalized HF and those followed-up at HF clinics. The Italian Working Group on Heart Failure has drafted a guidance document for the organisation of a national HF care network. Aims of the document are to describe tasks and requirements of the different health system points of contact for HF patients, and to define how diagnosis, management and care processes should be documented and shared among health-care professionals. The document classifies HF outpatient clinics in three groups: (i) community HF clinics, devoted to management of stable patients in strict liaison with primary care, periodic re-evaluation of emerging clinical needs and prompt treatment of impending destabilizations, (ii) hospital HF clinics, that target both new onset and chronic HF patients for diagnostic assessment, treatment planning and early post-discharge follow-up. They act as main referral for general internal medicine units and community clinics, and (iii) advanced HF clinics, directed at patients with severe disease or persistent clinical instability, candidates to advanced treatment options such as heart transplant or mechanical circulatory support. Those different types of HF clinics are integrated in a dedicated network for management of HF patients on a regional basis, according to geographic features. By sharing predefined protocols and communication systems, these HF networks integrate multi-professional providers to ensure continuity of care and patient empowerment. In conclusion, This guidance document details roles and interactions of cardiology specialists, so as to best exploit the added value of their input in the care of HF patients and is intended to promote a more efficient and effective organization of HF services.
Keywords: Chronic care model; Clinical competence; Disease networks; Heart failure; Outpatient clinics.
Figures
Similar articles
-
[ANMCO/SIC Consensus document: The heart failure network: organization of outpatient care].G Ital Cardiol (Rome). 2016 Jul-Aug;17(7-8):570-93. doi: 10.1714/2330.25052. G Ital Cardiol (Rome). 2016. PMID: 27571334 Italian.
-
[Questionnaire survey of the management of heart failure in the Marche Region, Italy].G Ital Cardiol (Rome). 2010 Mar;11(3):239-45. G Ital Cardiol (Rome). 2010. PMID: 20550065 Italian.
-
Heart failure outpatient clinics resources in Italy: a viewpoint of Italian Society of Cardiology organization.Heart Fail Rev. 2025 May;30(3):505-513. doi: 10.1007/s10741-024-10480-0. Epub 2025 Jan 8. Heart Fail Rev. 2025. PMID: 39777583 Free PMC article. Review.
-
[ANMCO/FADOI/SIAARTI/SIC/SIMG/SIMI/SIMEU consensus document: The clinical care pathway of acute heart failure patients from symptom onset to discharge from the emergency department].G Ital Cardiol (Rome). 2019 May;20(5):289-334. doi: 10.1714/3151.31321. G Ital Cardiol (Rome). 2019. PMID: 31066371 Italian.
-
[The ANMCO (National Association of Hospital Cardiologists) in a changing health care system. Consensus development of the Organizing Symposium of the XXXI National Congress of Cardiology--ANMCO; Florence, May 21, 2000].Ital Heart J Suppl. 2000 Dec;1(12):1533-44. Ital Heart J Suppl. 2000. PMID: 11221582 Review. Italian.
Cited by
-
The role of bioelectrical phase angle in patients with heart failure.Rev Endocr Metab Disord. 2023 Jun;24(3):465-477. doi: 10.1007/s11154-022-09757-2. Epub 2022 Oct 25. Rev Endocr Metab Disord. 2023. PMID: 36282462 Free PMC article. Review.
-
Cardiovascular Effects of Stimulators of Soluble Guanylate Cyclase Administration: A Meta-analysis of Randomized Controlled Trials.Curr Atheroscler Rep. 2024 May;26(5):177-187. doi: 10.1007/s11883-024-01197-4. Epub 2024 Apr 2. Curr Atheroscler Rep. 2024. PMID: 38564140
-
Determinants of survival in patients with chronic heart failure: a population-based study in Reggio Emilia, Italy.ESC Heart Fail. 2023 Dec;10(6):3646-3655. doi: 10.1002/ehf2.14557. Epub 2023 Oct 5. ESC Heart Fail. 2023. PMID: 37798817 Free PMC article.
-
Health schools as an organizational form of realization of the "life course health development" concept.J Med Life. 2021 May-Jun;14(3):413-418. doi: 10.25122/jml-2021-1127. J Med Life. 2021. PMID: 34377210 Free PMC article. Clinical Trial.
-
Understanding networks in low-and middle-income countries' health systems: A scoping review.PLOS Glob Public Health. 2023 Jan 11;3(1):e0001387. doi: 10.1371/journal.pgph.0001387. eCollection 2023. PLOS Glob Public Health. 2023. PMID: 36962859 Free PMC article.
References
-
- Norton C, Georgiopoulou VV, Kalogeropoulos AP, Butler J.. Epidemiology and cost of advanced heart failure. Prog Cardiovasc Dis 2011;54:78–78. - PubMed
-
- Cook C, Cole G, Asaria P, Jabbour R, Francis DP.. The annual global economic burden of heart failure. Int J Cardiol 2014;171:368–376. - PubMed
-
- Jong P, Gong Y, Liu PP, Austin PC, Lee DS, Tu JV.. Care and outcomes of patients newly hospitalized for heart failure in the community treated by cardiologists compared with other specialists. Circulation 2003;108:184–191. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous