Impact of Age on Scleral Buckling Surgery for Rhegmatogenous Retinal Detachment
- PMID: 28752694
- PMCID: PMC5540988
- DOI: 10.3341/kjo.2016.0024
Impact of Age on Scleral Buckling Surgery for Rhegmatogenous Retinal Detachment
Abstract
Purpose: The purpose of this study is to investigate new prognostic factors in associated with primary anatomical failure after scleral buckling (SB) for uncomplicated rhegmatogenous retinal detachment (RRD).
Methods: The medical records of patients with uncomplicated RRD treated with SB were retrospectively reviewed. Eyes with known prognostic factors for RRD, such as fovea-on, proliferative vitreoretinopathy, pseudophakia, aphakia, multiple breaks, or media opacity, were excluded. Analysis was performed to find correlations between anatomical success and various parameters, including age.
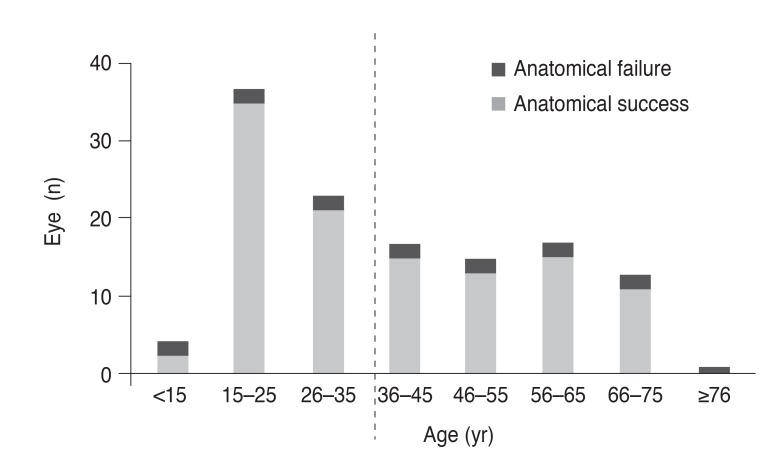
Results: This study analyzed 127 eyes. Binary logistic regression analysis revealed that older age (≥35) was the sole independent prognostic factor (odds ratio, 3.5; p = 0.022). Older age was correlated with worse preoperative visual acuity (p < 0.001), shorter symptom duration (p < 0.001), presence of a large tear (p < 0.001), subretinal fluid drainage (p < 0.001), postoperative macular complications (p = 0.048), and greater visual improvement (p = 0.003).
Conclusions: Older age (≥35) was an independent prognostic factor for primary anatomical failure in SB for uncomplicated RRD. The distinguished features of RRD between older and younger patients suggest that vitreous liquefaction and posterior vitreous detachment are important features associated with variation in surgical outcomes.
Keywords: Age; Prognostic factor; Rhegmatogenous retinal detachment; Scleral buckling; Vitreous.
© 2017 The Korean Ophthalmological Society
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Pastor JC, Fernandez I, Rodriguez de la Rua E, et al. Surgical outcomes for primary rhegmatogenous retinal detachments in phakic and pseudophakic patients: the Retina 1 Project. Report 2. Br J Ophthalmol. 2008;92:378–382. - PubMed
-
- Afrashi F, Akkin C, Egrilmez S, et al. Anatomic outcome of scleral buckling surgery in primary rhegmatogenous retinal detachment. Int Ophthalmol. 2005;26:77–81. - PubMed
-
- Heimann H, Bartz-Schmidt KU, Bornfeld N, et al. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment: a prospective randomized multicenter clinical study. Ophthalmology. 2007;114:2142–2154. - PubMed
-
- Sharma YR, Karunanithi S, Azad RV, et al. Functional and anatomic outcome of scleral buckling versus primary vitrectomy in pseudophakic retinal detachment. Acta Ophthalmol Scand. 2005;83:293–297. - PubMed
-
- Feltgen N, Heimann H, Hoerauf H, et al. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment study (SPR study): risk assessment of anatomical outcome. SPR study report no. 7. Acta Ophthalmol. 2013;91:282–287. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical