

[Establishment of mouse endometrial injury model by curettage or coagulation]
- PMID: 28752711
- PMCID: PMC10397007
- DOI: 10.3785/j.issn.1008-9292.2017.04.11
[Establishment of mouse endometrial injury model by curettage or coagulation]
Abstract
Objective: To establish mouse endometrial injury model by curettage or coagulation. Methods: Female ICR mice were randomly allocated into 2 groups: in curettage group, a blunt 20G needle was inserted in one uterine horn with 0.05 megapascals negative pressure; in coagulation group, one uterine horn was coagulated using a monopolar electric needle with 0.5 watts power. In both groups the contra-lateral uterine horn was used as control. The morphological changes and thickness of endometrium were evaluated 1 week after operation. The endometrial samples were taken on d4 of pregnancy, and the expressions of endometrial receptivity-related cytokines were examined. The number of implanted embryos on each side of uterus was calculated on d10 of pregnancy. Results: There was no difference in operation time between 2 groups. In both groups, the endometrial glands and stroma were significantly reduced, and the endometrial thickness was also significantly decreased on injury side compared to contra-lateral horn. However, local injury was more severe in coagulation group, uterine obliteration and hydrops were developed in 2 mice of coagulation group, and none in curettage group. The expressions of leukemia inhibitory factor (LIF) and oncostatin M (OSM) were significantly reduced on injured side in both groups compared to opposite side; however, the expression of LIF and OSM in curettage group was higher than that in coagulation group. The numbers of implanted embryos were decreased in both groups on injured side compared to opposite side, and fetal death was only observed in coagulation group. Conclusion: Both curettage and coagulation can make injury on mouse endometrium, impair endometrial receptivity and reduce fertility. Curettage can cause moderate injury, and coagulation may lead to more severe injury.
目的: 比较吸宫和电凝两种方法造成小鼠子宫内膜损伤模型的特点。
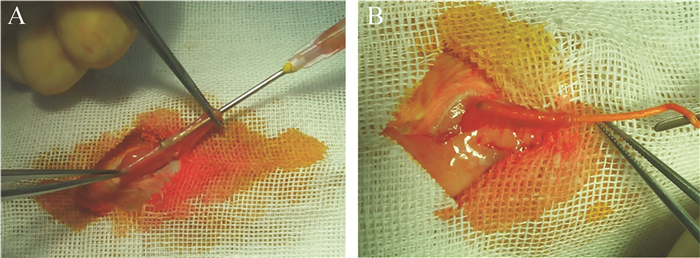
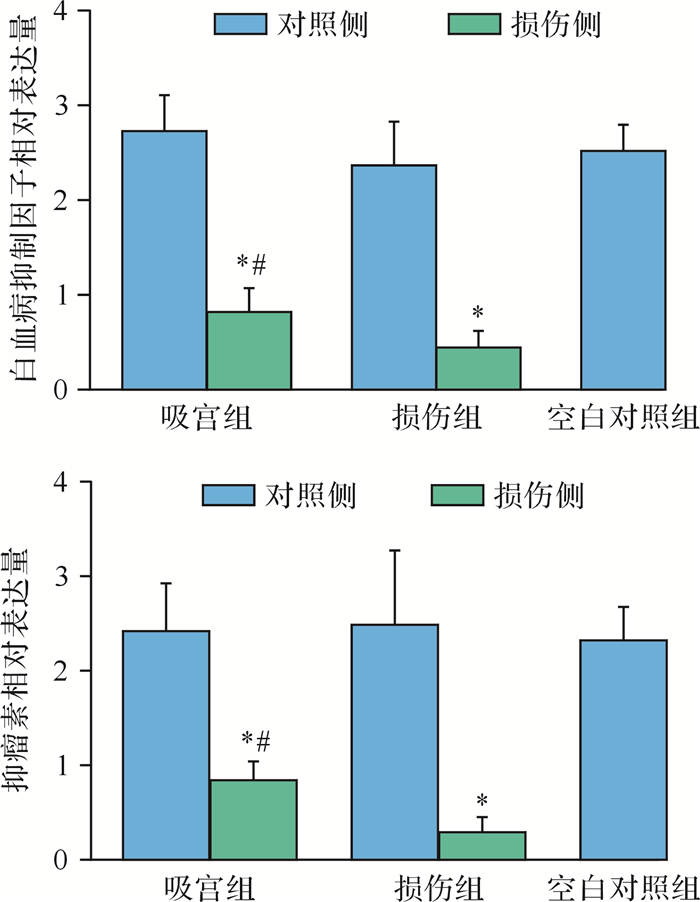
方法: 吸宫组采用自制20 G针头插入ICR小鼠一侧宫腔,以0.05 MPa负压全面吸宫1周;电凝组采用自制单极电针以0.5 W功率迅速电凝损伤子宫腔。均以对侧子宫为对照,对照仅插入针头或电针后退出。比较平均手术时间、术后单层子宫内膜厚度、妊娠4 d子宫内膜容受性相关因子的表达情况、妊娠10 d胎鼠数差别。其中HE染色观察子宫内膜组织形态学改变,蛋白质印迹法检测子宫内膜白血病抑制因子和抑瘤素M的表达。
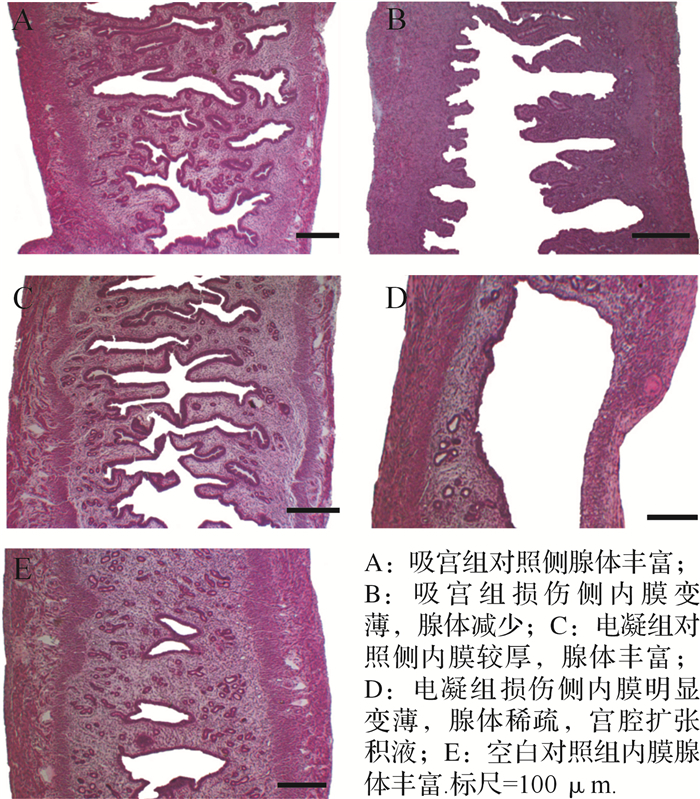
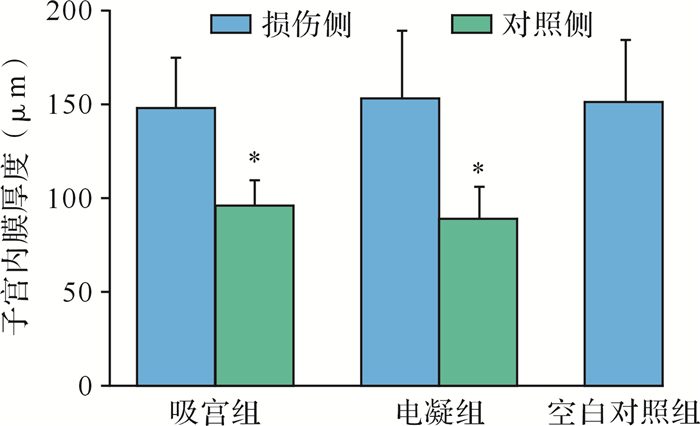
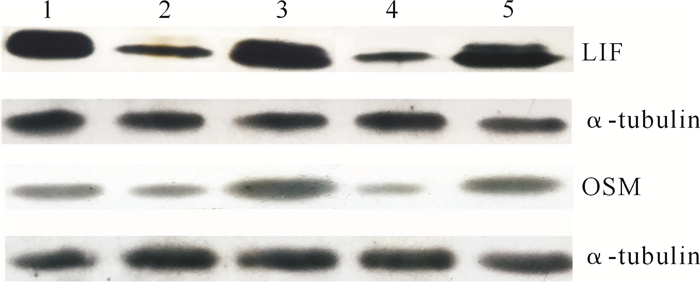
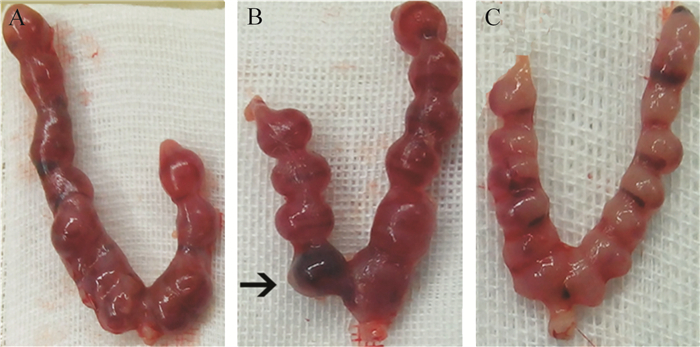
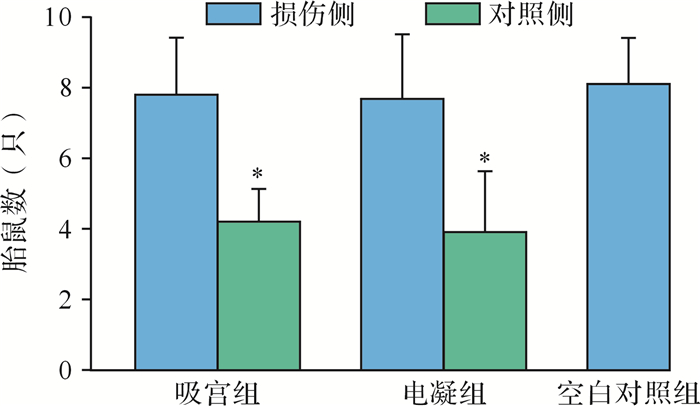
结果: 吸宫组平均手术时间(10.2±1.3)min,电凝组平均手术时间(10.1±1.5)min,差异无统计学意义( P > 0.05)。吸宫组损伤侧宫腔无封闭现象,电凝组有2只小鼠存在宫腔局部封闭、远段积水。损伤侧子宫内膜厚度吸宫组(96.1±13.2)μm,电凝组(88.9±16.8)μm,均比对照侧子宫减小(均 P < 0.01)。损伤侧子宫内膜白血病抑制因子和抑瘤素M的表达吸宫组高于电凝组,但两组损伤侧表达均低于对照侧(均 P < 0.01)。吸宫组损伤侧平均胎鼠数目(4.2±0.9)只,电凝组损伤侧平均胎鼠数目(3.9±1.7)只,均较对照侧下降(均 P < 0.01)。电凝组损伤侧还可见胎鼠死亡现象。
结论: 吸宫和电凝均可造成小鼠子宫内膜损伤,导致子宫内膜容受性下降和生育力受损。电凝损伤更符合重度宫腔粘连特征,而吸宫损伤可能更适用于轻中度宫腔粘连研究。
References
-
- HOOKER A, FRAENK D, BROLMANN H, et al. Prevalence of intrauterine adhesions after termination of pregnancy: a systematic review. Eur J Contracept Reprod Health Care. 2016;21(4):329–335. doi: 10.1080/13625187.2016.1199795. [HOOKER A, FRAENK D, BROLMANN H, et al. Prevalence of intrauterine adhesions after termination of pregnancy: a systematic review[J]. Eur J Contracept Reprod Health Care, 2016, 21(4):329-335.] - DOI - PubMed
-
- HEALY M W, SCHEXNAYDER B, CONNELL M T, et al. Intrauterine adhesion prevention after hysteroscopy: a systematic review and meta-analysis. Am J Obstet Gynecol. 2016;215(3):267–275. doi: 10.1016/j.ajog.2016.05.001. [HEALY M W, SCHEXNAYDER B, CONNELL M T, et al. Intrauterine adhesion prevention after hysteroscopy: a systematic review and meta-analysis[J]. Am J Obstet Gynecol, 2016, 215(3):267-275.e7.] - DOI - PubMed
-
- CONFORTI A, ALVIGGI C, MOLLO A, et al. The management of Asherman syndrome: a review of literature. Reprod Biol Endocrinol. 2013;11:118. doi: 10.1186/1477-7827-11-118. [CONFORTI A, ALVIGGI C, MOLLO A, et al. The management of Asherman syndrome: a review of literature[J]. Reprod Biol Endocrinol, 2013, 11:118.] - DOI - PMC - PubMed
-
- DILBAZ B, AKPINAR F, ALTINBAS S, et al. Reproductive outcome of patients with Asherman's syndrome after hysteroscopic adhesiolysis. https://link.springer.com/article/10.1007/s00404-009-1117-x. J Minim Invasive Gynecol. 2015;22(6S):S185–S186. [DILBAZ B, AKPINAR F, ALTINBAS S, et al. Reproductive outcome of patients with Asherman's syndrome after hysteroscopic adhesiolysis[J]. J Minim Invasive Gynecol, 2015, 22(6S):S185-S186.] - PubMed
-
- 曲 军英, 吕 一帆, 林 茵, et al. 建立小鼠子宫内膜损伤模型的研究. http://www.cnki.com.cn/Article/CJFDTOTAL-FJYD201101012.htm. 福建医科大学学报. 2011;45(1):34–36. [曲军英, 吕一帆, 林茵, 等.建立小鼠子宫内膜损伤模型的研究[J].福建医科大学学报, 2011, 45(1):34-36.]
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
