

Clinical outcomes and mortality before and after implementation of a pediatric sepsis protocol in a limited resource setting: A retrospective cohort study in Bangladesh
- PMID: 28753618
- PMCID: PMC5533322
- DOI: 10.1371/journal.pone.0181160
Clinical outcomes and mortality before and after implementation of a pediatric sepsis protocol in a limited resource setting: A retrospective cohort study in Bangladesh
Abstract
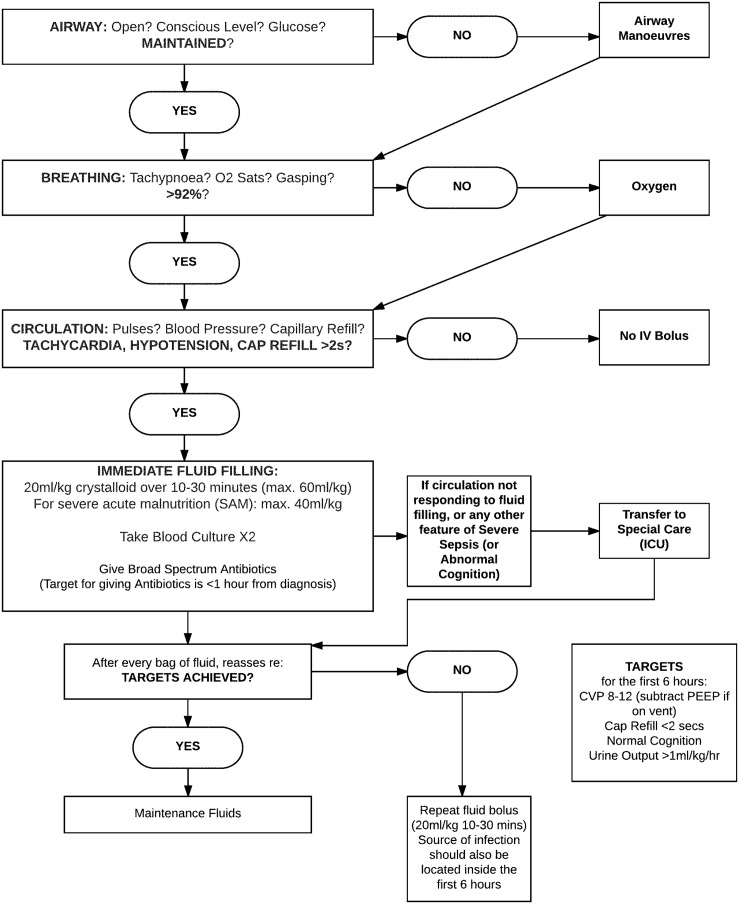
Background: Pediatric sepsis has a high mortality rate in limited resource settings. Sepsis protocols have been shown to be a cost-effective strategy to improve morbidity and mortality in a variety of populations and settings. At Dhaka Hospital in Bangladesh, mortality from pediatric sepsis in high-risk children previously approached 60%, which prompted the implementation of an evidenced-based protocol in 2010. The clinical effectiveness of this protocol had not been measured. We hypothesized that implementation of a pediatric sepsis protocol improved clinical outcomes, including reducing mortality and length of hospital stay.
Materials and methods: This was a retrospective cohort study of children 1-59 months old with a diagnosis of sepsis, severe sepsis or septic shock admitted to Dhaka Hospital from 10/25/2009-10/25/2011. The primary outcome was inpatient mortality pre- and post-protocol implementation. Secondary outcomes included fluid overload, heart failure, respiratory insufficiency, length of hospital stay, and protocol compliance, as measured by antibiotic and fluid bolus administration within 60 minutes of hospital presentation.
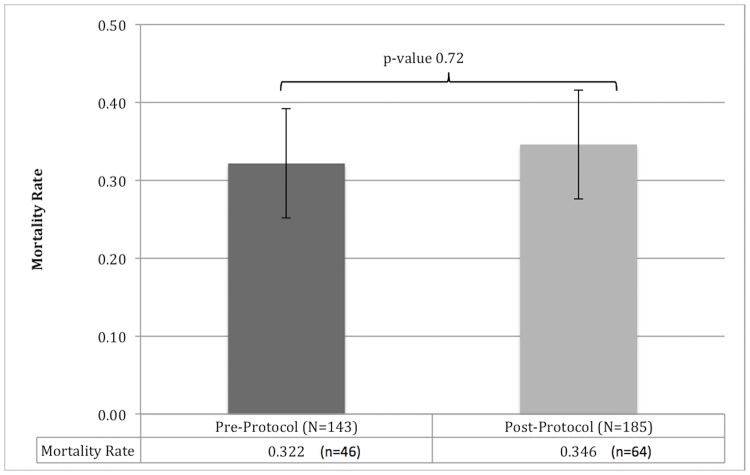
Results: 404 patients were identified by a key-word search of the electronic medical record; 328 patients with a primary diagnosis of sepsis, severe sepsis, or septic shock were included (143 pre- and185 post-protocol) in the analysis. Pre- and post-protocol mortality were similar and not statistically significant (32.17% vs. 34.59%, p = 0.72). The adjusted odds ratio (AOR) for post-protocol mortality was 1.55 (95% CI, 0.88-2.71). The odds for developing fluid overload were significantly higher post-protocol (AOR 3.45, 95% CI, 2.04-5.85), as were the odds of developing heart failure (AOR 4.52, 95% CI, 1.43-14.29) and having a longer median length of stay (AOR 1.81, 95% CI 1.10-2.96). There was no statistically significant difference in respiratory insufficiency (pre- 65.7% vs. post- 70.3%, p = 0.4) or antibiotic administration between the cohorts (pre- 16.08% vs. post- 12.43%, p = 0.42).
Conclusions: Implementation of a pediatric sepsis protocol did not improve all-cause mortality or length of stay and may have been associated with increased fluid overload and heart failure during the study period in a large, non-governmental hospital in Bangladesh. Similar rates of early antibiotic administration may indicate poor protocol compliance. Though evidenced-based protocols are a potential cost-effective strategy to improve outcomes, future studies should focus on optimal implementation of context-relevant sepsis protocols in limited resource settings.
Conflict of interest statement
Figures


References
-
- UNICEF. Committing to Child Survival: A Promise Renewed. Progress Report 2015. New York, NY: UNICEF; 2015.
-
- Kissoon N, Carcillo JA, Espinosa V, Argent A, Devictor D, Madden M, et al. World Federation of Pediatric Intensive Care and Critical Care Societies: Global Sepsis Initiative. Pediatric critical care medicine: a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies. 2011;12(5):494–503. - PubMed
-
- Watson RS, Carcillo JA. Scope and epidemiology of pediatric sepsis. Pediatric critical care medicine: a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies. 2005;6(3 Suppl):S3–5. - PubMed
-
- Wiens MO, Kumbakumba E, Kissoon N, Ansermino JM, Ndamira A, Larson CP. Pediatric sepsis in the developing world: challenges in defining sepsis and issues in post-discharge mortality. Clinical epidemiology. 2012;4:319–25. doi: 10.2147/CLEP.S35693 - DOI - PMC - PubMed
-
- Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, Scherag A, et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). Jama. 2016;315(8):762–74. doi: 10.1001/jama.2016.0288 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
