

Collaborative update of a rule-based expert system for HIV-1 genotypic resistance test interpretation
- PMID: 28753637
- PMCID: PMC5533429
- DOI: 10.1371/journal.pone.0181357
Collaborative update of a rule-based expert system for HIV-1 genotypic resistance test interpretation
Abstract
Introduction: HIV-1 genotypic resistance test (GRT) interpretation systems (IS) require updates as new studies on HIV-1 drug resistance are published and as treatment guidelines evolve.
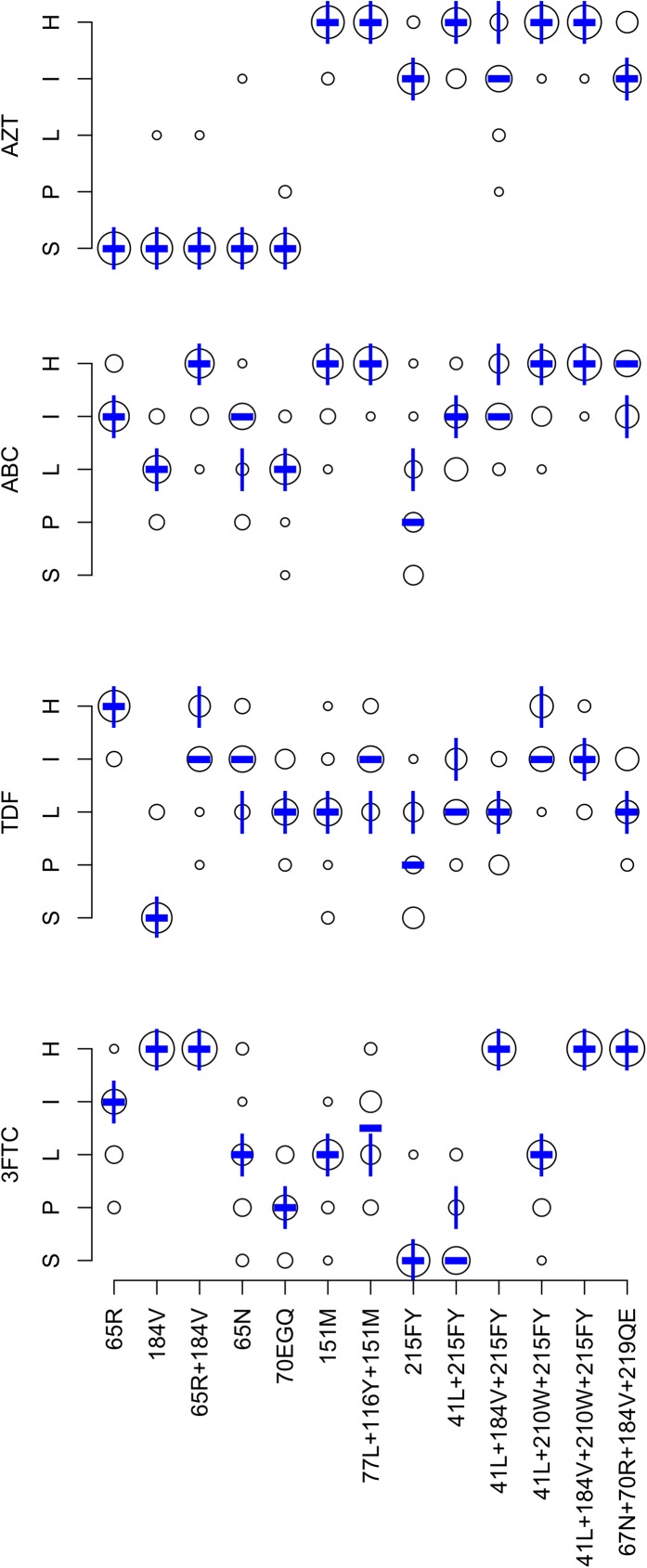
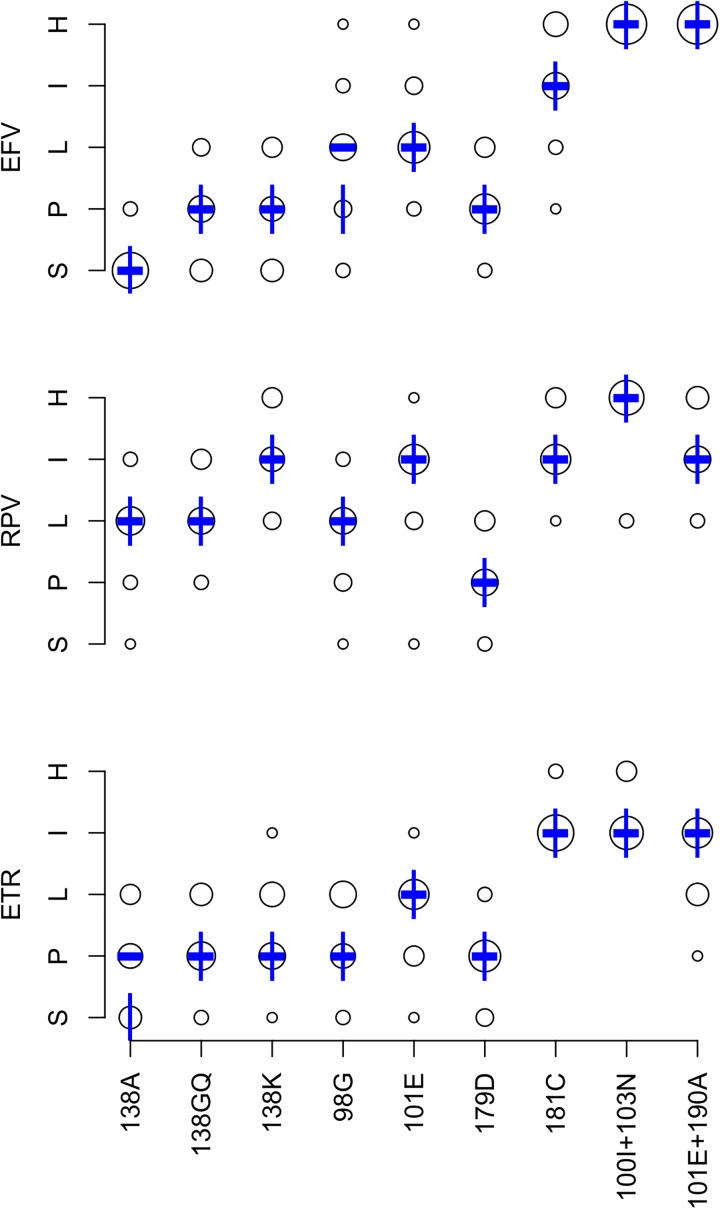
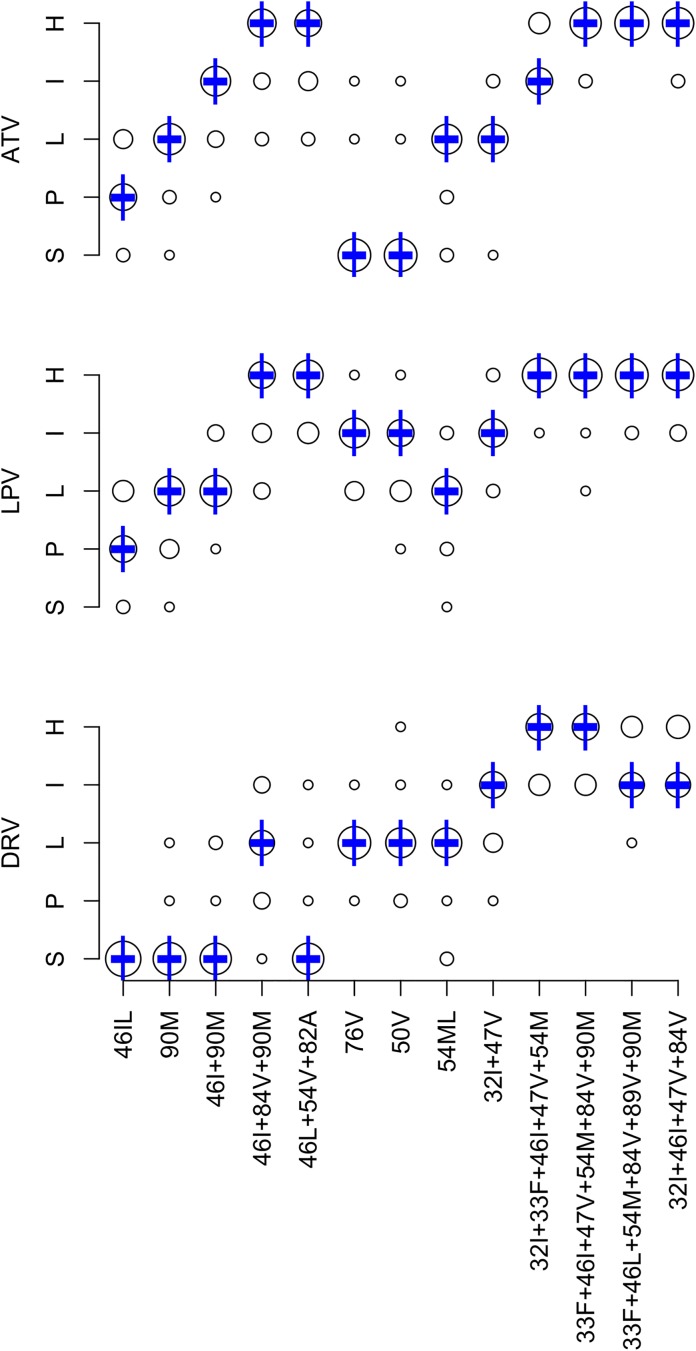
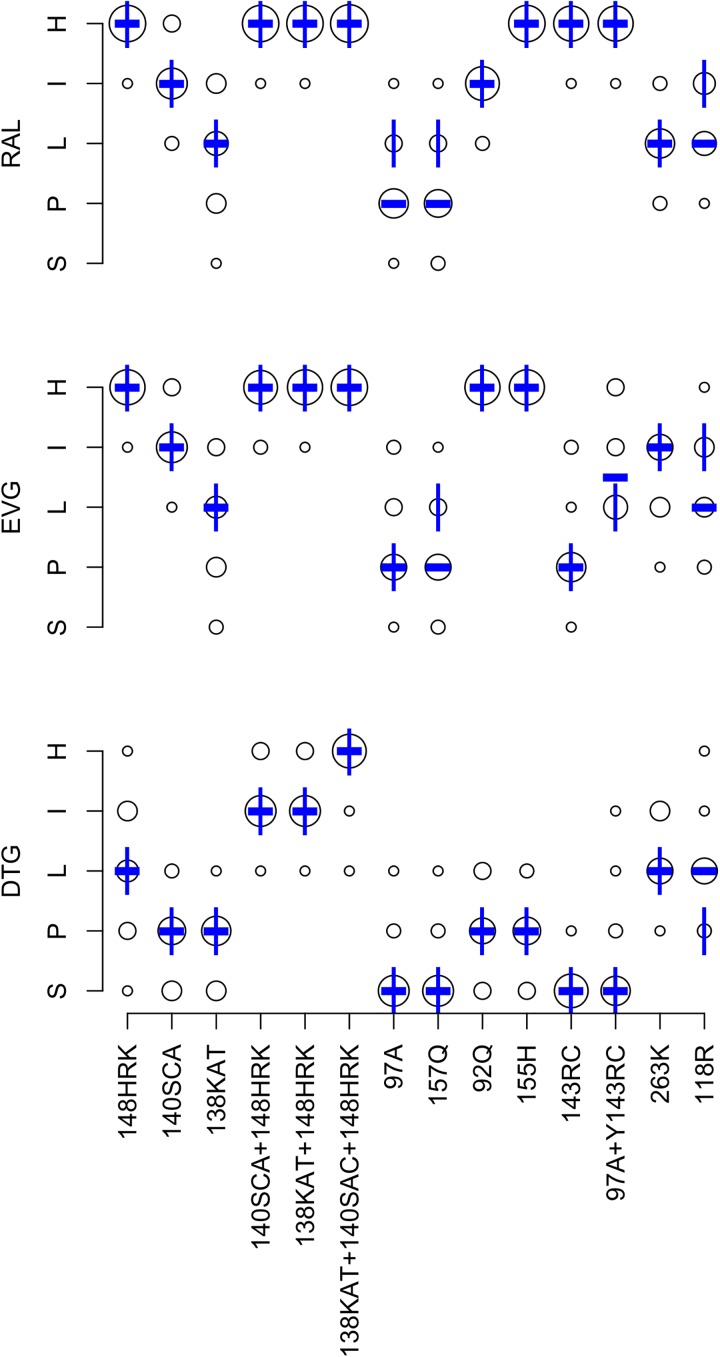
Methods: An expert panel was created to provide recommendations for the update of the Stanford HIV Drug Resistance Database (HIVDB) GRT-IS. The panel was polled on the ARVs to be included in a GRT report, and the drug-resistance interpretations associated with 160 drug-resistance mutation (DRM) pattern-ARV combinations. The DRM pattern-ARV combinations included 52 nucleoside RT inhibitor (NRTI) DRM pattern-ARV combinations (13 patterns x 4 NRTIs), 27 nonnucleoside RT inhibitor (NNRTI) DRM pattern-ARV combinations (9 patterns x 3 NNRTIs), 39 protease inhibitor (PI) DRM pattern-ARV combinations (13 patterns x 3 PIs) and 42 integrase strand transfer inhibitor (INSTI) DRM pattern-ARV combinations (14 patterns x 3 INSTIs).
Results: There was universal agreement that a GRT report should include the NRTIs lamivudine, abacavir, zidovudine, emtricitabine, and tenofovir disoproxil fumarate; the NNRTIs efavirenz, etravirine, nevirapine, and rilpivirine; the PIs atazanavir/r, darunavir/r, and lopinavir/r (with "/r" indicating pharmacological boosting with ritonavir or cobicistat); and the INSTIs dolutegravir, elvitegravir, and raltegravir. There was a range of opinion as to whether the NRTIs stavudine and didanosine and the PIs nelfinavir, indinavir/r, saquinavir/r, fosamprenavir/r, and tipranavir/r should be included. The expert panel members provided highly concordant DRM pattern-ARV interpretations with only 6% of NRTI, 6% of NNRTI, 5% of PI, and 3% of INSTI individual expert interpretations differing from the expert panel median by more than one resistance level. The expert panel median differed from the HIVDB 7.0 GRT-IS for 20 (12.5%) of the 160 DRM pattern-ARV combinations including 12 NRTI, two NNRTI, and six INSTI pattern-ARV combinations. Eighteen of these differences were updated in HIVDB 8.1 GRT-IS to reflect the expert panel median. Additionally, HIVDB users are now provided with the option to exclude those ARVs not considered to be universally required.
Conclusions: The HIVDB GRT-IS was updated through a collaborative process to reflect changes in HIV drug resistance knowledge, treatment guidelines, and expert opinion. Such a process broadens consensus among experts and identifies areas requiring further study.
Conflict of interest statement
Figures
Similar articles
-
Trends in HIV-1 Drug Resistance Mutations from a U.S. Reference Laboratory from 2006 to 2017.AIDS Res Hum Retroviruses. 2019 Aug;35(8):698-709. doi: 10.1089/AID.2019.0063. Epub 2019 Jul 10. AIDS Res Hum Retroviruses. 2019. PMID: 31169022
-
First case of Dolutegravir and Darunavir/r multi drug-resistant HIV-1 in Cameroon following exposure to Raltegravir: lessons and implications in the era of transition to Dolutegravir-based regimens.Antimicrob Resist Infect Control. 2020 Aug 26;9(1):143. doi: 10.1186/s13756-020-00799-2. Antimicrob Resist Infect Control. 2020. PMID: 32843050 Free PMC article.
-
Predictive Efficacy of Dual Therapies Combining Integrase Strand Transfer Inhibitors with Second-Generation Non-Nucleoside Reverse Transcriptase Inhibitors Following HIV-1 Treatment Failure in Cameroon: Implications for the Use of a Long-Acting Therapeutic Strategy in Low- and Middle-Income Countries.Viruses. 2024 Nov 29;16(12):1853. doi: 10.3390/v16121853. Viruses. 2024. PMID: 39772163 Free PMC article.
-
Abacavir/dolutegravir/lamivudine single-tablet regimen: a review of its use in HIV-1 infection.Drugs. 2015 Apr;75(5):503-14. doi: 10.1007/s40265-015-0361-6. Drugs. 2015. PMID: 25698454 Review.
-
Comparative efficacy and safety of dolutegravir relative to common core agents in treatment-naïve patients infected with HIV-1: a systematic review and network meta-analysis.BMC Infect Dis. 2019 May 30;19(1):484. doi: 10.1186/s12879-019-3975-6. BMC Infect Dis. 2019. PMID: 31146698 Free PMC article.
Cited by
-
A Robotic Cognitive Architecture for Slope and Dam Inspections.Sensors (Basel). 2020 Aug 15;20(16):4579. doi: 10.3390/s20164579. Sensors (Basel). 2020. PMID: 32824151 Free PMC article.
-
Comparison of an In Vitro Diagnostic Next-Generation Sequencing Assay with Sanger Sequencing for HIV-1 Genotypic Resistance Testing.J Clin Microbiol. 2018 May 25;56(6):e00105-18. doi: 10.1128/JCM.00105-18. Print 2018 Jun. J Clin Microbiol. 2018. PMID: 29618499 Free PMC article.
-
Human Immunodeficiency Virus Type 1 Drug Resistance Mutations Update.J Infect Dis. 2017 Dec 1;216(suppl_9):S843-S846. doi: 10.1093/infdis/jix398. J Infect Dis. 2017. PMID: 28968669 Free PMC article.
-
Archived rilpivirine-associated resistance mutations among ART-naive and virologically suppressed people living with HIV-1 subtype C in Botswana: implications for cabotegravir/rilpivirine use.J Antimicrob Chemother. 2023 Oct 3;78(10):2489-2495. doi: 10.1093/jac/dkad258. J Antimicrob Chemother. 2023. PMID: 37585352 Free PMC article.
-
Incorporating temporal dynamics of mutations to enhance the prediction capability of antiretroviral therapy's outcome for HIV-1.Bioinformatics. 2024 Jun 3;40(6):btae327. doi: 10.1093/bioinformatics/btae327. Bioinformatics. 2024. PMID: 38775719 Free PMC article.
References
-
- Vandamme AM, Camacho RJ, Ceccherini-Silberstein F, de Luca A, Palmisano L, Paraskevis D, et al. European recommendations for the clinical use of HIV drug resistance testing: 2011 update. AIDS reviews. 2011;13(2):77–108. . - PubMed
-
- Liu TF, Shafer RW. Web resources for HIV type 1 genotypic-resistance test interpretation. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2006;42(11):1608–18. doi: 10.1086/503914 ; PubMed Central PMCID: PMCPMC2547473. - DOI - PMC - PubMed
-
- Tang MW, Liu TF, Shafer RW. The HIVdb system for HIV-1 genotypic resistance interpretation. Intervirology. 2012;55(2):98–101. doi: 10.1159/000331998 . - DOI - PMC - PubMed
-
- Monogram Biosciences. PhenoSense HIV Drug Resistance Assay Report Template (last accessed May 18, 2017). https://wwwmonogrambiocom/sites/monogrambio/files/imce/uploads/PS_report.... 2017.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
