

Comparison of neuropsychiatric symptoms and diffusion tensor imaging correlates among patients with subcortical ischemic vascular disease and Alzheimer's disease
- PMID: 28754095
- PMCID: PMC5534111
- DOI: 10.1186/s12883-017-0911-5
Comparison of neuropsychiatric symptoms and diffusion tensor imaging correlates among patients with subcortical ischemic vascular disease and Alzheimer's disease
Erratum in
-
Correction to: Comparison of neuropsychiatric symptoms and diffusion tensor imaging correlates among patients with subcortical ischemic vascular disease and Alzheimer's disease.BMC Neurol. 2017 Oct 2;17(1):189. doi: 10.1186/s12883-017-0969-0. BMC Neurol. 2017. PMID: 28969595 Free PMC article. No abstract available.
Abstract
Background: The causes of behavioral and psychological symptoms of dementia (BPSD) vary according to the dementia subtype and associated neuropathology. The present study aimed to (i) compare BPSD between patients with subcortical ischemic vascular disease (SIVD) and Alzheimer's disease (AD) across stages, and (ii) explore the associations with diffusion tensor imaging (DTI) in the corpus callosum (CC) and other major fibers.
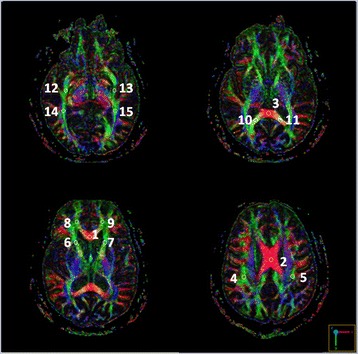
Methods: Twenty-four patients with SIVD and 32 with AD were recruited. Four domains of the Neuropsychiatric Inventory (NPI) (hyperactivity, psychosis, affective, and apathy) and two DTI parameters [fractional anisotropy (FA) and mean diffusivity (MD)] within the genu, body (BCC), and splenium (SCC) of the CC and other major fibers were assessed.
Results: Overall, the patients with clinical dementia rating (CDR) 1 ~ 2 had higher scores in apathy domain than those with CDR0.5. Among those with CDR1 ~ 2, SIVD had higher scores in apathy domain than AD. MD values in the BCC/SCC were positively correlated with total NPI score and psychosis, hyperactivity, and apathy domains. FA values in the SCC were inversely correlated with total NPI score and psychosis domain. The correlations were modified by age, the CASI, and CDR scores. Stepwise linear regression models suggested that FA value within the left superior longitudinal fasciculus predicted the hyperactivity domain. MD value within the SCC/left uncinate fasciculus and FA value within the GCC/left forceps major predicted the psychosis domain. MD value within the right superior longitudinal fasciculus and CDR predicted the apathy domain. Further analysis suggested distinct patterns of regression models between SIVD and AD patients.
Conclusion: White matter integrity within the BCC/SCC had associations with multi-domains of BPSD. Our study also identified important roles of regions other than the CC to individual domain of BPSD, including the left superior longitudinal fasciculus to the hyperactivity domain, the left uncinate fasciculus/forceps major to the psychosis domain, and the right superior longitudinal fasciculus to the apathy domain. The neuronal substrates in predicting BPSD were different between SIVD and AD patients. Of note, apathy, which was more profound in SIVD, was associated with corresponding fiber disconnection in line with dementia severity and global cognition decline.
Keywords: Alzheimer’s disease; Apathy; Behavioral and psychological symptoms of dementia; Corpus callosum; Diffusion tensor imaging; Neuropsychiatric inventory; Psychosis; Subcortical ischemic vascular disease.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of our hospital (REC 103–14). All participants and caregivers provided their written informed consent to participate in this study.
Consent for publication
Not applicable [The data contain no information of individual identity].
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Effectiveness of diffusion tensor imaging in differentiating early-stage subcortical ischemic vascular disease, Alzheimer's disease and normal ageing.PLoS One. 2017 Apr 7;12(4):e0175143. doi: 10.1371/journal.pone.0175143. eCollection 2017. PLoS One. 2017. PMID: 28388630 Free PMC article.
-
The value of diffusion tensor imaging in the differential diagnosis of subcortical ischemic vascular dementia and Alzheimer's disease in patients with only mild white matter alterations on T2-weighted images.Acta Radiol. 2012 Apr 1;53(3):312-7. doi: 10.1258/ar.2011.110272. Epub 2012 Mar 13. Acta Radiol. 2012. PMID: 22416261
-
Quantitative measurement to evaluate morphological changes of the corpus callosum in patients with subcortical ischemic vascular dementia.Acta Radiol. 2015 Feb;56(2):214-8. doi: 10.1177/0284185114520863. Epub 2014 Jan 20. Acta Radiol. 2015. PMID: 24445093
-
The role of diffusion tensor imaging and fractional anisotropy in the evaluation of patients with idiopathic normal pressure hydrocephalus: a literature review.Neurosurg Focus. 2016 Sep;41(3):E12. doi: 10.3171/2016.6.FOCUS16192. Neurosurg Focus. 2016. PMID: 27581308 Review.
-
Imaging Alzheimer's genetic risk using diffusion MRI: A systematic review.Neuroimage Clin. 2020;27:102359. doi: 10.1016/j.nicl.2020.102359. Epub 2020 Jul 22. Neuroimage Clin. 2020. PMID: 32758801 Free PMC article.
Cited by
-
Multiparameter resting-state functional magnetic resonance imaging as an indicator of neuropsychological changes in Binswanger's disease with mild cognitive impairment.Front Aging Neurosci. 2025 Feb 10;17:1522591. doi: 10.3389/fnagi.2025.1522591. eCollection 2025. Front Aging Neurosci. 2025. PMID: 39995946 Free PMC article.
-
Empirical support for the vascular apathy hypothesis: A structured review.Int J Geriatr Psychiatry. 2020 Jan;35(1):3-11. doi: 10.1002/gps.5217. Epub 2019 Oct 30. Int J Geriatr Psychiatry. 2020. PMID: 31617249 Free PMC article.
-
Dissociable Functional Brain Networks Associated With Apathy in Subcortical Ischemic Vascular Disease and Alzheimer's Disease.Front Aging Neurosci. 2022 Feb 3;13:717037. doi: 10.3389/fnagi.2021.717037. eCollection 2021. Front Aging Neurosci. 2022. PMID: 35185511 Free PMC article.
-
Neuroanatomical associations of depression, anxiety and apathy neuropsychiatric symptoms in patients with Alzheimer's disease.Acta Neurol Belg. 2021 Dec;121(6):1469-1480. doi: 10.1007/s13760-020-01349-8. Epub 2020 Apr 21. Acta Neurol Belg. 2021. PMID: 32319015
-
White matter tract microstructure and cognitive performance after transient ischemic attack.PLoS One. 2020 Oct 23;15(10):e0239116. doi: 10.1371/journal.pone.0239116. eCollection 2020. PLoS One. 2020. PMID: 33095770 Free PMC article.
References
-
- Finkel SI, Burns A. BPSD consensus statement. Int Psychogeriatric Asso. 1999.
-
- Fuh JL. Study of behavioral and psychological symptoms of dementia in Taiwan. Acta Neurol Taiwanica. 2006;15:154–160. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
