

Provider and Practice Factors Associated With Emergency Physicians' Being Named in a Malpractice Claim
- PMID: 28754358
- PMCID: PMC5785561
- DOI: 10.1016/j.annemergmed.2017.06.023
Provider and Practice Factors Associated With Emergency Physicians' Being Named in a Malpractice Claim
Abstract
Study objective: We examine the association between emergency physician characteristics and practice factors with the risk of being named in a malpractice claim.
Methods: We used malpractice claims along with provider, operational, and jurisdictional data from a national emergency medicine group (87 emergency departments [EDs] in 15 states from January 1, 2010, to June 30, 2014) to assess the relationship between individual physician and practice variables and being named in a malpractice claim. Individual and practice factors included years in practice, emergency medicine board certification, visit admission rate, relative value units generated per hour, total patients treated as attending physician of record, working at multiple facilities, working primarily overnight shifts, patient experience data percentile, and state malpractice environment. We assessed the relationship between emergency physician and practice variables and malpractice claims, using logistic regression.
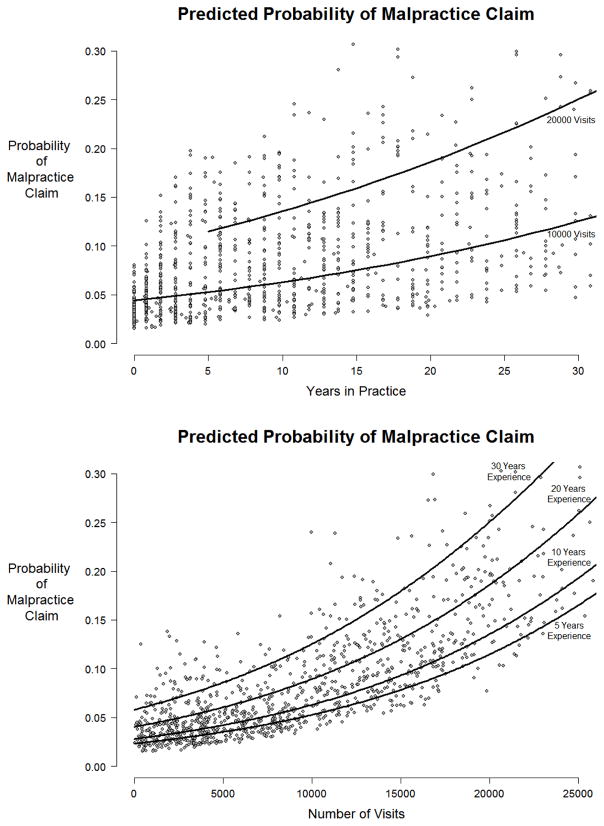
Results: Of 9,477,150 ED visits involving 1,029 emergency physicians, there were 98 malpractice claims against 90 physicians (9%). Increasing total number of years in practice (adjusted odds ratio 1.04; 95% confidence interval 1.02 to 1.06) and higher visit volume (adjusted odds ratio 1.09 per 1,000 visits; 95% confidence interval 1.05 to 1.12) were associated with being named in a malpractice claim. No other factors were associated with malpractice claims.
Conclusion: In this sample of emergency physicians, 1 in 11 were named in a malpractice claim during 4.5 years. Total number of years in practice and visit volume were the only identified factors associated with being named, suggesting that exposure to higher patient volumes and longer practice experience are the primary contributors to malpractice risk.
Copyright © 2017 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Malpractice Claims: It's a Crapshoot-Time to Stop the Self-Blame and Ask Different Questions.Ann Emerg Med. 2018 Feb;71(2):165-167. doi: 10.1016/j.annemergmed.2017.09.013. Epub 2017 Nov 6. Ann Emerg Med. 2018. PMID: 29107402 No abstract available.
-
Medicolegal Data Empower Better and Safer Health Care.Ann Emerg Med. 2018 Sep;72(3):326-327. doi: 10.1016/j.annemergmed.2018.04.013. Ann Emerg Med. 2018. PMID: 30144872 No abstract available.
-
In reply.Ann Emerg Med. 2018 Sep;72(3):327-328. doi: 10.1016/j.annemergmed.2018.04.011. Ann Emerg Med. 2018. PMID: 30144873 No abstract available.
References
-
- Bishop TF, Federman AD, Keyhani S. Physicians’ views on defensive medicine: a national survey. Arch Intern Med. 2010 Jun 28;170(12):1081–1083. - PubMed
-
- Sanbar SS, Firestone MH. [Accessed September 27, 2016];Medical Malpractice Stress Syndrome. http://www.acep.org/uploadedFiles/ACEP/Professional_Development/Faculty_....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
