

Lung Function and Incident Kidney Disease: The Atherosclerosis Risk in Communities (ARIC) Study
- PMID: 28754455
- PMCID: PMC5651181
- DOI: 10.1053/j.ajkd.2017.05.021
Lung Function and Incident Kidney Disease: The Atherosclerosis Risk in Communities (ARIC) Study
Abstract
Background: Reduced lung function is associated with clinical outcomes such as cardiovascular disease. However, little is known about its association with incident end-stage renal disease (ESRD) and chronic kidney disease (CKD).
Study design: Prospective cohort study.
Setting & participants: 14,946 participants aged 45 to 64 years at baseline (1987-1989) in the Atherosclerosis Risk in Communities (ARIC) Study (45.0% men and 25.2% black), with follow-up through 2012.
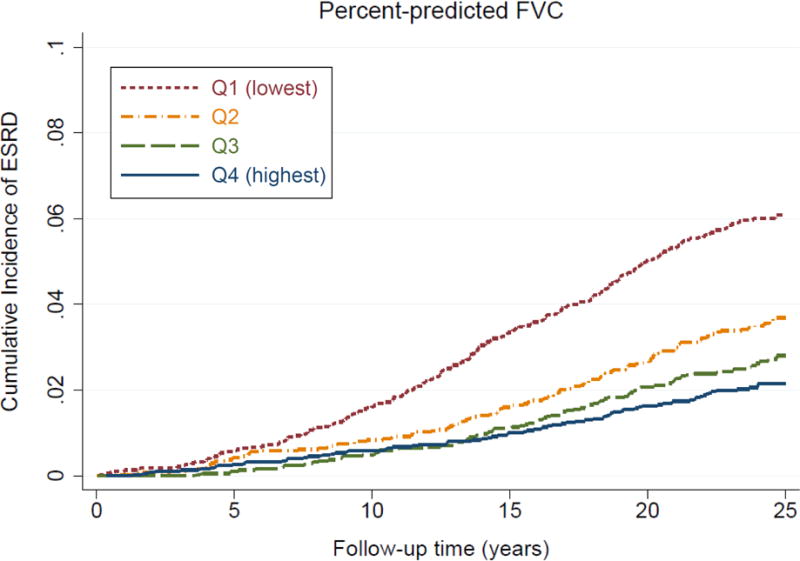
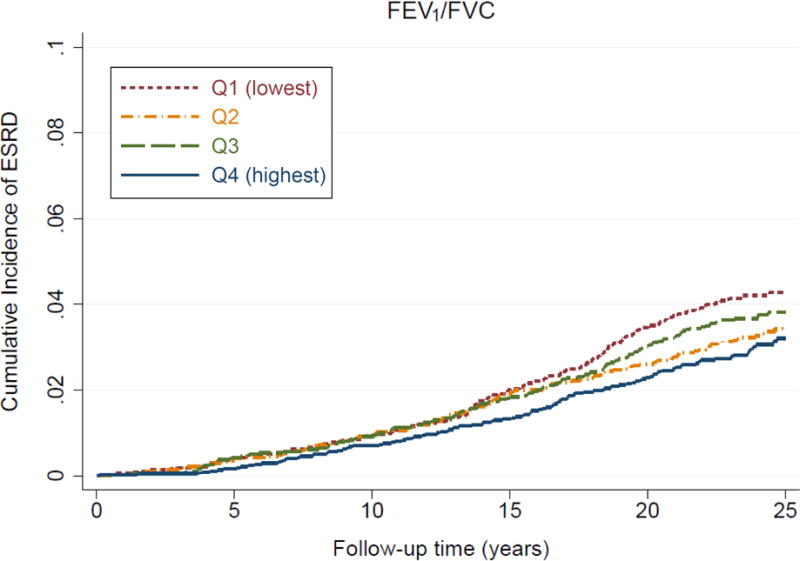
Predictors: Race- and sex-specific quartiles of percent-predicted forced vital capacity (FVC) and the proportion of forced expiratory volume in 1 second of expiration to FVC (FEV1/FVC) at baseline determined with spirometry.
Outcomes: Incident ESRD (defined here as renal replacement therapy or death due to CKD) as the primary outcome and incident CKD (defined here as ESRD, ≥25% decline in estimated glomerular filtration rate to a level <60mL/min/1.73m2, or CKD-related hospitalizations/deaths) as the secondary outcome.
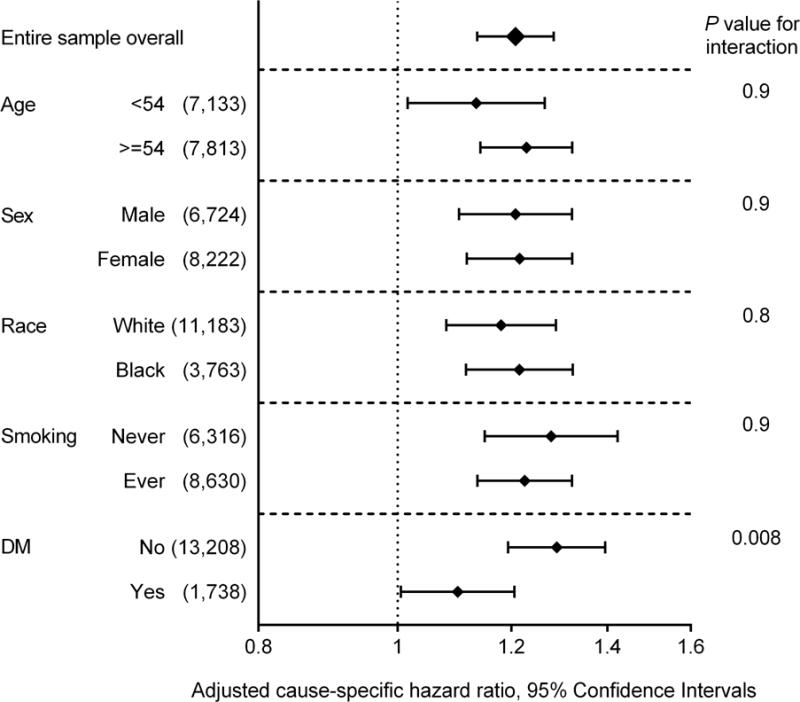
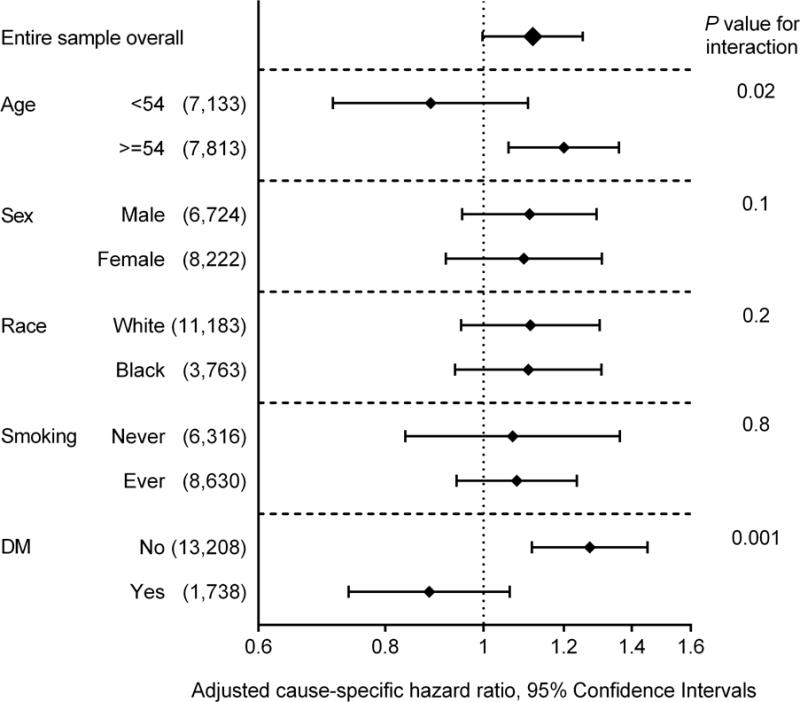
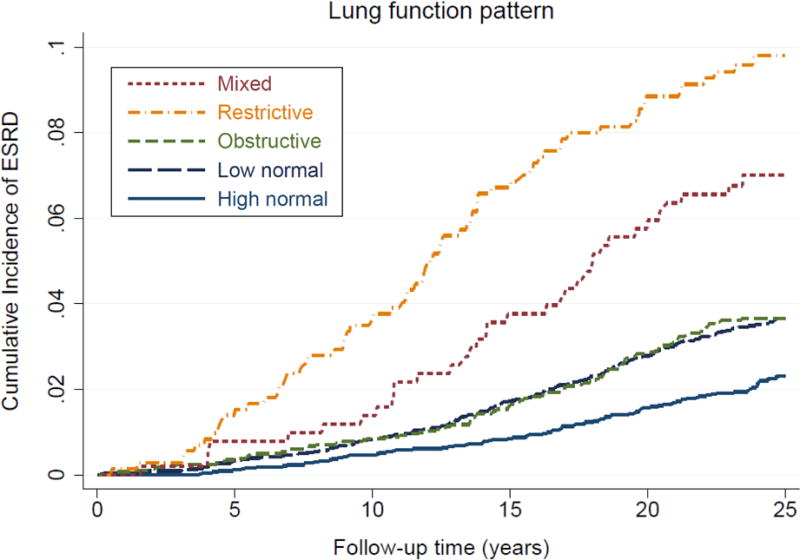
Results: During a median follow-up of 23.6 years, 526 (3.5%) participants developed ESRD. After adjusting for potential confounders, the cause-specific HR of incident ESRD for the lowest (vs highest) quartile was 1.72 (95% CI, 1.31-2.26) for percent-predicted FVC and 1.33 (95% CI, 1.03-1.73) for FEV1/FVC. Compared to a high-normal lung function pattern, a mixed pattern (ie, percent-predicted FVC<80% and FEV1/FVC<70%; 3.4% of participants) demonstrated the highest adjusted cause-specific HR of ESRD at 2.28 (95% CI, 1.50-3.45), followed by the restrictive pattern (ie, percent-predicted FVC<80% and FEV1/FVC≥70%; 4.8% of participants) at 2.03 (95% CI, 1.47-2.81), obstructive pattern (ie, percent-predicted FVC≥80% and FEV1/FVC<70%; 18.9% of participants) at 1.47 (95% CI, 1.09-1.99), and low-normal pattern (ie, percent-predicted FVC 80%-<100% and FEV1/FVC≥70%, or percent-predicted FVC≥80% and FEV1/FVC 70%-<75%; 44.3% of participants) at 1.21 (95% CI, 0.94-1.55). Similar associations were seen with incident CKD.
Limitations: Limited number of participants with moderate/severe lung dysfunction and spirometry only at baseline.
Conclusions: Reduced lung function, particularly lower percent-predicted FVC, is independently associated with CKD progression. Our findings suggest a potential pathophysiologic contribution of reduced lung function to the development of CKD and a need for monitoring kidney function in persons with reduced lung function.
Keywords: Atherosclerosis Risk in Communities (ARIC) Study; Lung function; chronic kidney disease (CKD); end-stage renal disease (ESRD); estimated glomerular filtration rate (eGFR); obstructive lung function; restrictive lung function; spirometry.
Copyright © 2017 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
In line with AJKD’s procedures for potential conflicts of interest for editors, described in the Information for Authors & Journal policies, Health Equity Editor Carmen A. Peralta, MD, served as Acting Editor-in-Chief and handled the peer-review and decision-making processes.
Figures
References
-
- Mannino DM, Ford ES, Redd SC. Obstructive and restrictive lung disease and markers of inflammation: data from the Third National Health and Nutrition Examination. Am J Med. 2003;114(9):758–762. - PubMed
-
- Ford ES, Mannino DM, Wheaton AG, Giles WH, Presley-Cantrell L, Croft JB. Trends in the prevalence of obstructive and restrictive lung function among adults in the United States: findings from the National Health and Nutrition Examination surveys from 1988–1994 to 2007–2010. Chest. 2013;143(5):1395–1406. - PMC - PubMed
-
- Schunemann HJ, Dorn J, Grant BJ, Winkelstein W, Jr, Trevisan M. Pulmonary function is a long-term predictor of mortality in the general population: 29-year follow-up of the Buffalo Health Study. Chest. 2000;118(3):656–664. - PubMed
-
- Schroeder EB, Welch VL, Couper D, Nieto FJ, Liao D, Rosamond WD, Heiss G. Lung Function and Incident Coronary Heart Disease: The Atherosclerosis Risk in Communities Study. Am J Epidemiol. 2003;158(12):1171–1181. - PubMed
MeSH terms
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
