

Efficacy and Safety of Human Intravenous Immunoglobulin 10% (Panzyga®) in Patients with Primary Immunodeficiency Diseases: a Two-Stage, Multicenter, Prospective, Open-Label Study
- PMID: 28755067
- PMCID: PMC5554470
- DOI: 10.1007/s10875-017-0424-4
Efficacy and Safety of Human Intravenous Immunoglobulin 10% (Panzyga®) in Patients with Primary Immunodeficiency Diseases: a Two-Stage, Multicenter, Prospective, Open-Label Study
Abstract
Purpose: To assess the efficacy and safety of panzyga® (intravenous immunoglobulin 10%) in preventing serious bacterial infections (SBIs) in patients with primary immunodeficiency diseases (PIDs), a prospective, open-label, multicenter, phase 3 study and an open-label extension study were undertaken.
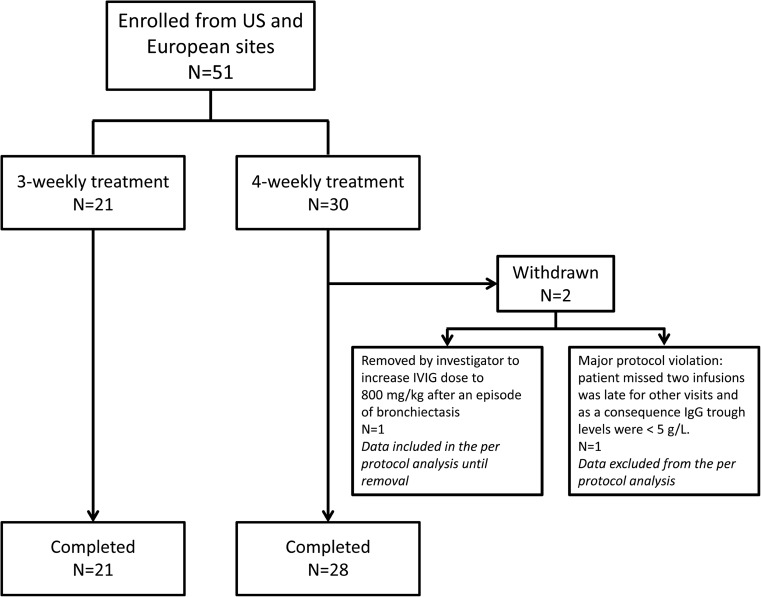
Methods: Initially, the study drug (infusion rate ≤0.08 mL/kg/min) was administered at intervals of 3 or 4 weeks for 12 months, followed by 3 months of panzyga® at infusion rates increasing from 0.08 to 0.14 mL/kg/min. The primary endpoint in the main study was the rate of SBIs per patient-year on treatment. Secondary outcomes included non-serious infections, work/school absence, episodes of fever, quality of life, and adverse events (AEs).
Results: The main study enrolled 51 patients (35% female, mean age 26.8 years), with 21 participating in the extension study. The rate of SBIs per patient-year was 0.08 in the total population; there were four SBIs in the 4-weekly treatment group (2/30 patients) and none in the 3-weekly group (n = 21). Compared with 4-weekly treatment, 3-weekly treatment was associated with a higher rate of upper respiratory tract infections (RTIs), ear infections, and work/school absences, but a lower rate of lower RTIs and fever. Treatment was generally well tolerated; no AE led to treatment withdrawal or death.
Conclusions: Overall, the use of panzyga® in patients with antibody-deficient PID was associated with a low rate of AEs and was effective in preventing SBIs, exceeding US FDA and European Medicines Agency recommendations for efficacy.
Keywords: Primary immunodeficiency diseases; intravenous immunoglobulin; panzyga®; serious bacterial infections.
Conflict of interest statement
M Borte’s institution has received research grant support from CSL Behring, Octapharma, and Baxalta, and he has participated in advisory boards for CSL Behring and Octapharma. IR Melamed has received research grant support from CSL Behring, Octapharma, Baxalta, and Bio Products Laboratories. B. Pyringer is an employee of Octapharma, Vienna, Austria. AP Knutsen has acted as a consultant for Baxalta, CSL, and Octapharma. HD Ochs has acted as consultant for Baxalta, CSL Behring, and Octapharma. RH Kobayashi has acted as a consultant for Baxalta, CSL, ADMA, and Octapharma. AL Kobayashi received grant support from Baxalta and Octapharma. JN Moy has received fees as a consultant for Grifols, Prometic, Octapharma, MacroCure, and Baxalta. G Pulka, S Gupta, M Strach, W Smits, and A Pituch-Noworolska have no conflicts of interest to declare. Open Access for this Article was funded by Octapharma.
Figures
References
-
- Picard C, Al-Herz W, Bousfiha A, Casanova JL, Chatila T, Conley ME, et al. Primary immunodeficiency diseases: an update on the classification from the International Union of Immunological Societies Expert Committee for Primary Immunodeficiency 2015. J Clin Immunol. 2015;35(8):696–726. doi: 10.1007/s10875-015-0201-1. - DOI - PMC - PubMed
-
- Berger M, Murphy E, Riley P, Bergman GE. Improved quality of life, immunoglobulin G levels, and infection rates in patients with primary immunodeficiency diseases during self-treatment with subcutaneous immunoglobulin G. South Med J. 2010;103(9):856–863. doi: 10.1097/SMJ.0b013e3181eba6ea. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
