

Chronic Remote Ischemic Conditioning Is Cerebroprotective and Induces Vascular Remodeling in a VCID Model
- PMID: 28755277
- PMCID: PMC5750336
- DOI: 10.1007/s12975-017-0555-1
Chronic Remote Ischemic Conditioning Is Cerebroprotective and Induces Vascular Remodeling in a VCID Model
Abstract
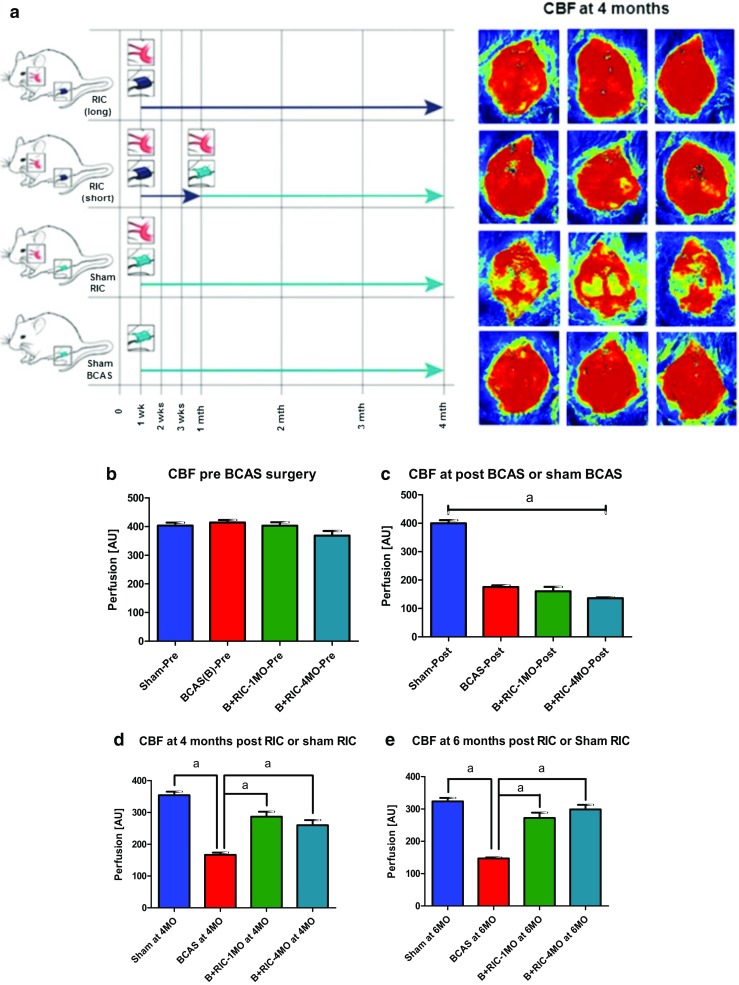
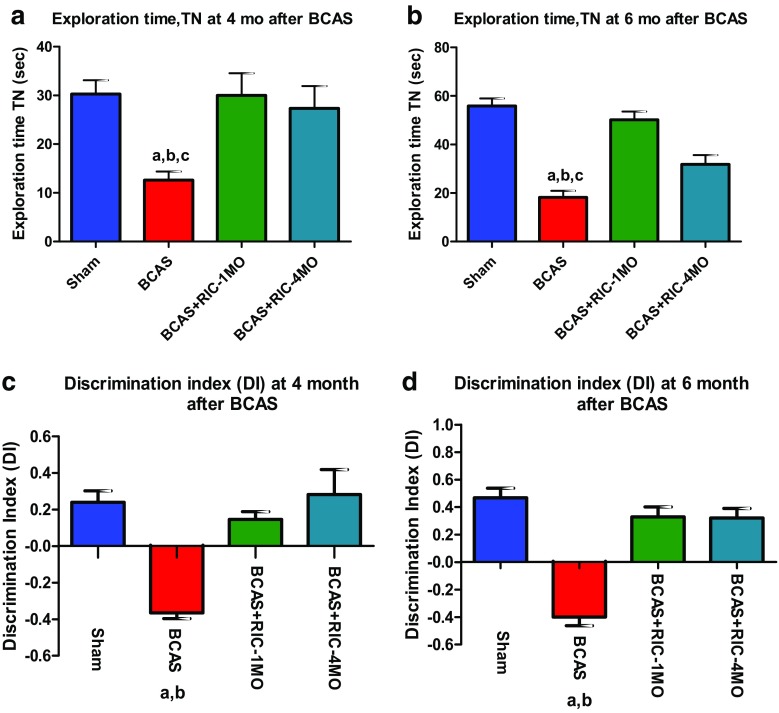
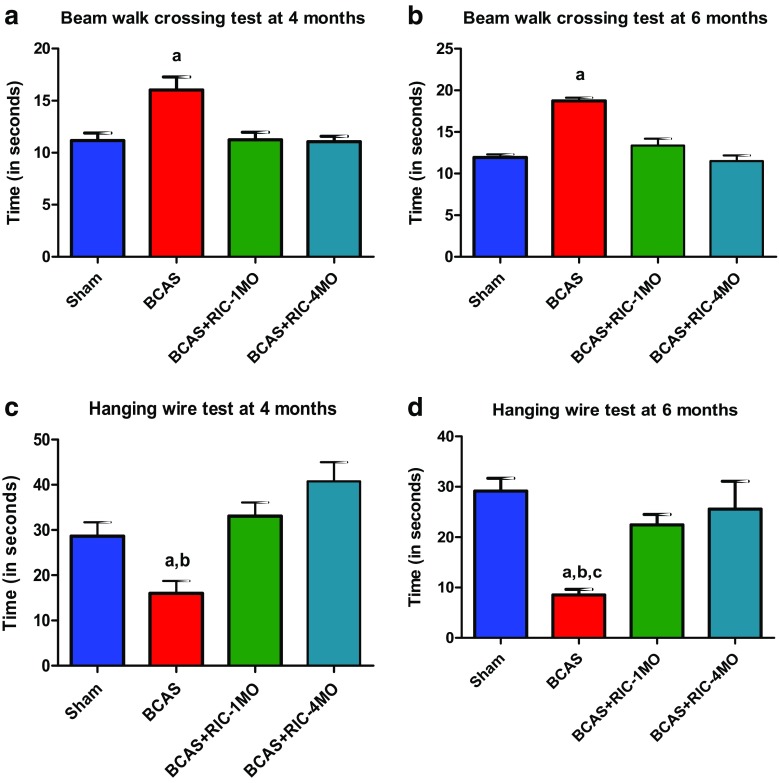
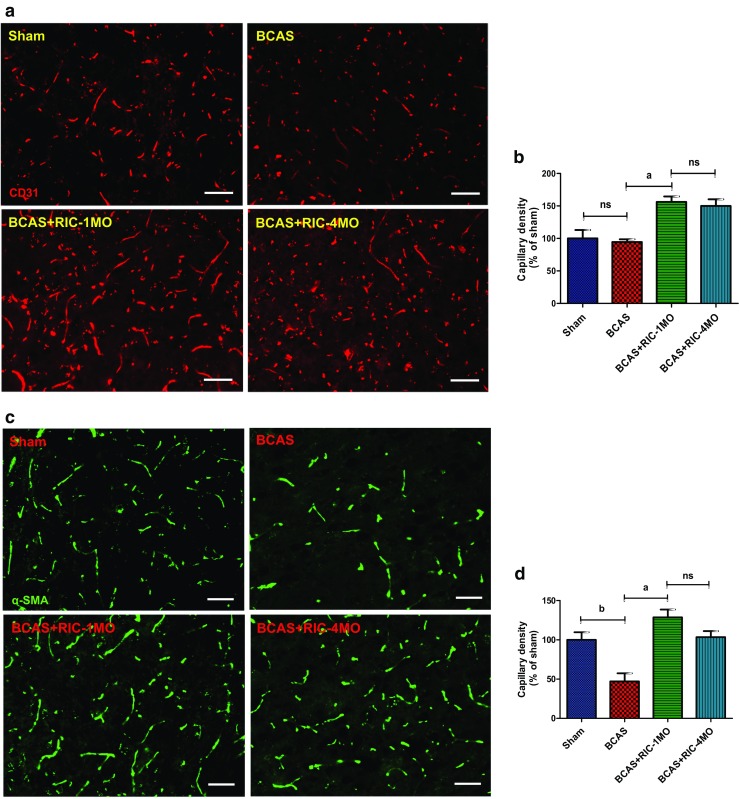
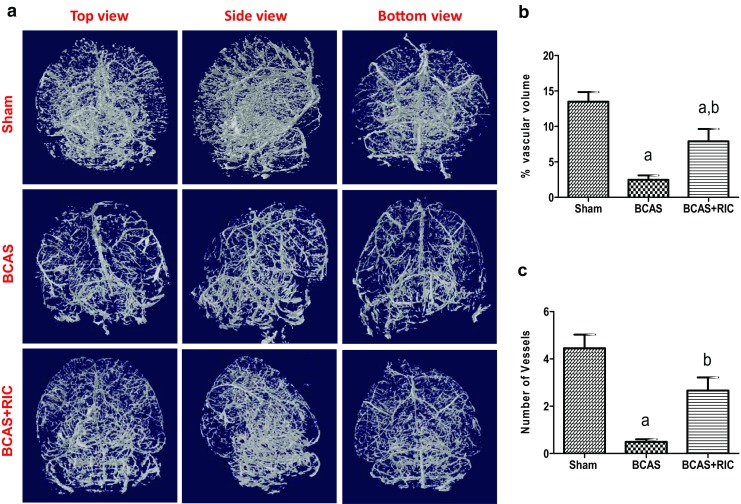
Vascular contributions to cognitive impairment and dementia (VCID) make up 50% of the cases of dementia. The purpose of this study was to determine the effect of chronic remote ischemic conditioning (C-RIC) on improving long-term (6 months) outcomes and cerebral blood flow (CBF) and collateral formation in a mouse model of VCID. Adult C57BL/6J male mice (10 weeks) were randomly assigned to four different groups: (1) sham-bilateral carotid artery stenosis (BCAS), (2) BCAS + sham RIC, (3) BCAS+C-RIC for 1 month (1MO), and (4) BCAS+C-RIC-4 months (4MO). CBF, cognitive impairment, and functional outcomes were performed up for 6 months after BCAS surgery. The expression of CD31, α-SMA, and myelin basic protein (MBP) was assessed by immunohistochemistry (IHC). Additional set of mice were randomized to sham, BCAS, and BCAS+C-RIC. The cerebrovascular angioarchitecture was studied with micro-CT. RIC therapy for either 1 or 4 months significantly improved CBF, new collateral formation, functional and cognitive outcomes, and prevented white matter damage. There was no difference between C-RIC for 1 or 4 months; IHC studies at 6 months showed an increase in brain CD31 and α-SMA expression indicating increased angiogenesis and MBP indicating preservation of white matter in animals receiving RIC. One month of daily RIC is as effective as 4 months of daily RIC in improving CBF, angiogenesis, and long-term functional outcomes (6 months) in a VCID model. This suggests that 1 month of RIC is sufficient to reduce cognitive impairment and induce beneficial cerebrovascular remodeling.
Keywords: Angiogenesis, collateral remodeling, white matter degeneration; Cerebral blood flow (CBF); Chronic remote ischemic conditioning (C-RIC); Vascular contributions to cognitive impairment and dementia (VCID).
Conflict of interest statement
Funding
This work was supported by the NIH/NINDS R21NS090609-01A1. We are special thankful to Mr. Richard Goodman, Hatteras Instruments, Cary, NC, in accepting a proposed design and making a multichannel non-invasive programmable remote ischemic conditioner and for a generous gift to our laboratory.
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All applicable institutional and national guidelines for the care and use of animals were followed.
Figures
References
-
- Corriveau RA, Bosetti F, Emr M, Gladman JT, Koenig JI, Moy CS, et al. The science of vascular contributions to cognitive impairment and dementia (VCID): a framework for advancing research priorities in the cerebrovascular biology of cognitive decline. Cell Mol Neurobiol. 2016;36(2):281–288. doi: 10.1007/s10571-016-0334-7. - DOI - PMC - PubMed
-
- Verdelho A, Madureira S, Ferro JM, Baezner H, Blahak C, Poggesi A, et al. Physical activity prevents progression for cognitive impairment and vascular dementia: results from the LADIS (Leukoaraiosis and Disability) study. Stroke. 2012;43(12):3331–3335. doi: 10.1161/STROKEAHA.112.661793. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
