

Association of Blood Pressure Control Level With Left Ventricular Morphology and Function and With Subclinical Cerebrovascular Disease
- PMID: 28757483
- PMCID: PMC5586460
- DOI: 10.1161/JAHA.117.006246
Association of Blood Pressure Control Level With Left Ventricular Morphology and Function and With Subclinical Cerebrovascular Disease
Abstract
Background: Left ventricular (LV) hypertrophy and subclinical cerebrovascular disease are early manifestations of cardiac and brain target organ damage caused by hypertension. This study aimed to investigate whether intensive office systolic blood pressure (SBP) control has beneficial effects on LV morphology and function and subclinical cerebrovascular disease in elderly patients with hypertension.
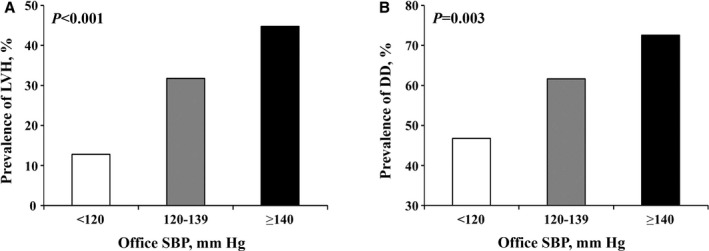
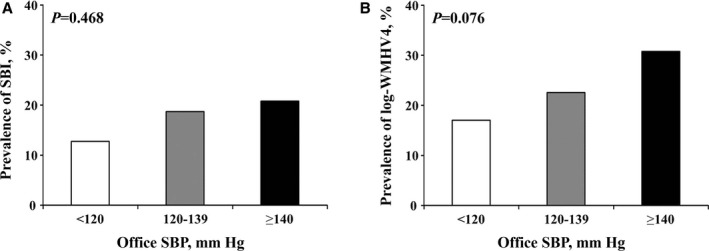
Methods and results: We examined 420 patients treated for hypertension without history of heart failure and stroke from the CABL (Cardiovascular Abnormalities and Brain Lesions) study. All patients underwent 2-dimensional echocardiographic examination and brain magnetic resonance imaging. Subclinical cerebrovascular disease was defined as silent brain infarcts and white matter hyperintensity volume. Patients were divided into 3 groups: SBP <120 mm Hg (intensive control); SBP 120 to 139 mm Hg (less intensive control); and SBP ≥140 mm Hg (uncontrolled). Prevalence of LV hypertrophy and diastolic dysfunction were lowest in the intensive control, intermediate in the less intensive control, and highest in the uncontrolled groups (12.8%, 31.8%, and 44.7%, respectively [P<0.001], for LV hypertrophy; 46.8%, 61.7%, and 72.6%, respectively [P=0.003], for diastolic dysfunction). Patients with less intensive SBP control had greater risk of LV hypertrophy than those with intensive control (adjusted odds ratio, 3.26; P=0.013). A similar trend was observed for LV diastolic dysfunction but did not reach statistical significance (adjusted odds ratio, 1.65; P=0.144). Conversely, intensive SBP control was not significantly associated with reduced risk of silent brain infarcts and white matter hyperintensity volume compared with less intensive control.
Conclusions: Compared with less intensive control, intensive SBP control may have a stronger beneficial effect on cardiac than cerebral subclinical disease.
Keywords: blood pressure; hypertension; left ventricular diastolic dysfunction; left ventricular hypertrophy; silent brain infarction.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Similar articles
-
Effect of Lower Blood Pressure Goals on Left Ventricular Structure and Function in Patients With Subclinical Hypertensive Heart Disease.Am J Hypertens. 2020 Sep 10;33(9):837-845. doi: 10.1093/ajh/hpaa108. Am J Hypertens. 2020. PMID: 32622346 Free PMC article. Clinical Trial.
-
Blood pressure variability in controlled and uncontrolled blood pressure and its association with left ventricular hypertrophy and diastolic function.J Hum Hypertens. 2016 Aug;30(8):483-7. doi: 10.1038/jhh.2015.106. Epub 2015 Oct 15. J Hum Hypertens. 2016. PMID: 26467817
-
Left ventricular mass-geometry and silent cerebrovascular disease: The Cardiovascular Abnormalities and Brain Lesions (CABL) study.Am Heart J. 2017 Mar;185:85-92. doi: 10.1016/j.ahj.2016.11.010. Epub 2016 Dec 21. Am Heart J. 2017. PMID: 28267479 Free PMC article.
-
Hypertension and Organ Damage in Women.High Blood Press Cardiovasc Prev. 2018 Sep;25(3):245-252. doi: 10.1007/s40292-018-0265-0. Epub 2018 Jun 26. High Blood Press Cardiovasc Prev. 2018. PMID: 29943358 Review.
-
Changes in left ventricular geometry during antihypertensive treatment.Pharmacol Res. 2018 Aug;134:193-199. doi: 10.1016/j.phrs.2018.06.026. Epub 2018 Jun 26. Pharmacol Res. 2018. PMID: 29959031 Review.
Cited by
-
Diastolic Blood Pressure Is Associated With Regional White Matter Lesion Load: The Northern Manhattan Study.Stroke. 2020 Feb;51(2):372-378. doi: 10.1161/STROKEAHA.119.025139. Epub 2020 Jan 8. Stroke. 2020. PMID: 31910743 Free PMC article.
-
Effect of Lower Blood Pressure Goals on Left Ventricular Structure and Function in Patients With Subclinical Hypertensive Heart Disease.Am J Hypertens. 2020 Sep 10;33(9):837-845. doi: 10.1093/ajh/hpaa108. Am J Hypertens. 2020. PMID: 32622346 Free PMC article. Clinical Trial.
-
Changes in Left Ventricular Mass and Geometry in the Older Adults: Role of Body Mass and Central Obesity.J Am Soc Echocardiogr. 2019 Oct;32(10):1318-1325. doi: 10.1016/j.echo.2019.05.018. Epub 2019 Jul 13. J Am Soc Echocardiogr. 2019. PMID: 31311705 Free PMC article.
-
Cross-Sectional Association Between Left Ventricular Geometric Patterns, Cortical Cerebral Microinfarcts, and Cognition.J Am Heart Assoc. 2025 Jan 21;14(2):e035522. doi: 10.1161/JAHA.124.035522. Epub 2025 Jan 17. J Am Heart Assoc. 2025. PMID: 39818861 Free PMC article.
-
Risk Factors in Optimal Management of Hypertension in Elderly Patients Following 2017 American College of Cardiology-American Heart Association Guidelines.J Prim Care Community Health. 2024 Jan-Dec;15:21501319241306897. doi: 10.1177/21501319241306897. J Prim Care Community Health. 2024. PMID: 39676249 Free PMC article.
References
-
- Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217–223. - PubMed
-
- Kannel WB, Gordon T, Schwartz MJ. Systolic versus diastolic blood pressure and risk of coronary heart disease. The Framingham study. Am J Cardiol. 1971;27:335–346. - PubMed
-
- Sagie A, Larson MG, Levy D. The natural history of borderline isolated systolic hypertension. N Engl J Med. 1993;329:1912–1917. - PubMed
-
- Frohlich ED. The heart in hypertension: unresolved conceptual challenges. Special lecture. Hypertension. 1988;11:I19–I24. - PubMed
-
- Weber KT. Cardioreparation in hypertensive heart disease. Hypertension. 2001;38:588–591. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
