

Lumbosacral Dorsal Rhizotomy for Spastic Cerebral Palsy: A Health Technology Assessment
- PMID: 28757906
- PMCID: PMC5515320
Lumbosacral Dorsal Rhizotomy for Spastic Cerebral Palsy: A Health Technology Assessment
Abstract
Background: Cerebral palsy, a spectrum of neuromuscular conditions caused by abnormal brain development or early damage to the brain, is the most common cause of childhood physical disability. Lumbosacral dorsal rhizotomy is a neurosurgical procedure that permanently decreases spasticity and is always followed by physical therapy. The objectives of this health technology assessment were to evaluate the clinical effectiveness, safety, cost effectiveness, and family perspectives of dorsal rhizotomy.
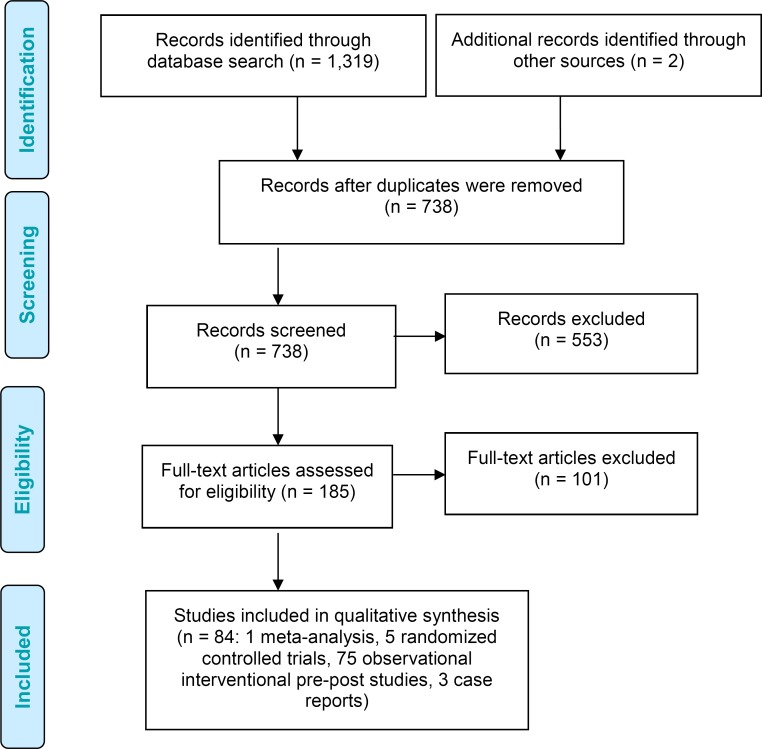
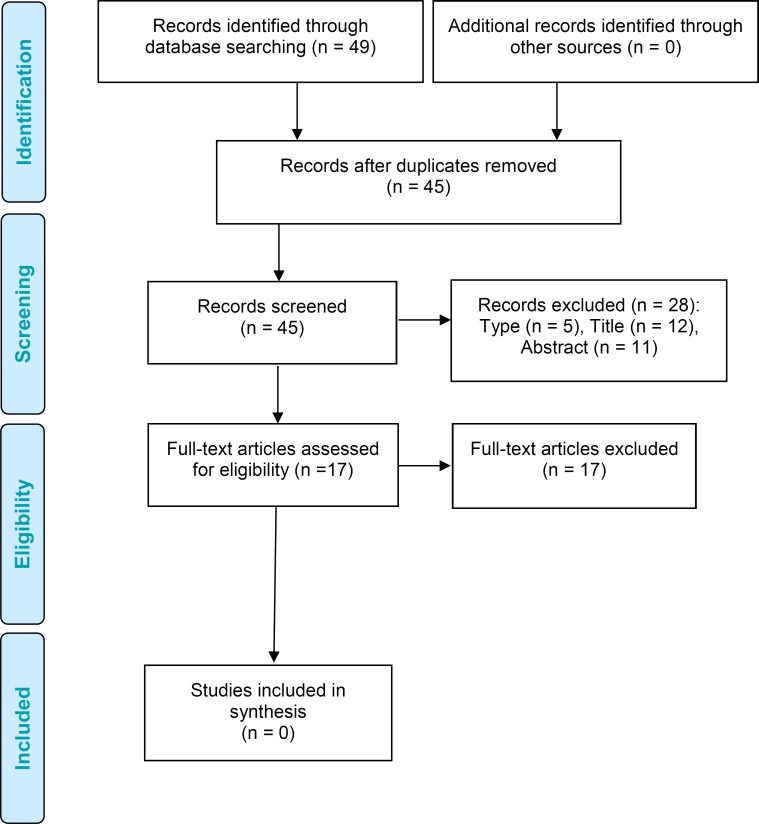
Methods: We performed a systematic literature search until December 2015 with auto-alerts until December 2016. Search strategies were developed by medical librarians, and a single reviewer reviewed the abstracts. The health technology assessment included a clinical review based on functional outcomes, safety, and treatment satisfaction; an economic study reviewing cost-effective literature; a budget impact analysis; and interviews with families evaluating the intervention.
Results: Eighty-four studies (1 meta-analysis, 5 randomized controlled studies [RCTs], 75 observational pre-post studies, and 3 case reports) were reviewed. A meta-analysis of RCTs involving dorsal rhizotomy and physical therapy versus physical therapy confirmed reduced lower-limb spasticity and increased gross motor function (4.5%, P = .002). Observational studies reported statistically significant improvements in gross motor function over 2 years or less (12 studies, GRADE moderate) and over more than 2 years (10 studies, GRADE moderate) as well as improvements in functional independence in the short term (10 studies, GRADE moderate) and long term (4 studies, GRADE low). Major operative complications, were infrequently reported (4 studies). Bony abnormalities and instabilities monitored radiologically in the spine (15 studies) and hip (8 studies) involved minimal or clinically insignificant changes after surgery. No studies evaluated the cost effectiveness of dorsal rhizotomy. The budget impact of funding dorsal rhizotomy for treatment of Ontario children with cerebral palsy was $1.3 million per year. Families reported perceived improvements in their children and expressed satisfaction with treatment. Ontario families reported inadequate medical information on benefits or risk to make an informed decision, enormous financial burdens, and lack rehabilitation support after surgery.
Conclusions: Lumbrosacral dorsal rhizotomy and physical therapy effectively reduces lower-limb spasticity in children with spastic cerebral palsy and significantly improves their gross motor function and functional independence. Major peri-operative complications were infrequently reported. Families reported perceived improvements with dorsal rhizotomy, and surgery and post-operative rehabilitation were intensive and demanding.
Figures

Similar articles
-
Long-term functional benefits of selective dorsal rhizotomy for spastic cerebral palsy.J Neurosurg Pediatr. 2013 Aug;12(2):142-50. doi: 10.3171/2013.4.PEDS12539. Epub 2013 May 28. J Neurosurg Pediatr. 2013. PMID: 23713680
-
Selective dorsal rhizotomy for the treatment of severe spastic cerebral palsy: efficacy and therapeutic durability in GMFCS grade IV and V children.Acta Neurochir (Wien). 2018 Apr;160(4):811-821. doi: 10.1007/s00701-017-3349-z. Epub 2017 Nov 7. Acta Neurochir (Wien). 2018. PMID: 29116382
-
Multidimensional outcome measure of selective dorsal rhizotomy in spastic cerebral palsy.Eur J Paediatr Neurol. 2014 Nov;18(6):704-13. doi: 10.1016/j.ejpn.2014.06.003. Epub 2014 Jun 11. Eur J Paediatr Neurol. 2014. PMID: 24954890
-
Upper-extremity spasticity and functionality after selective dorsal rhizotomy for cerebral palsy: a systematic review.J Neurosurg Pediatr. 2023 Sep 15;32(6):673-685. doi: 10.3171/2023.7.PEDS22526. Print 2023 Dec 1. J Neurosurg Pediatr. 2023. PMID: 37877954
-
Outcomes after selective dorsal rhizotomy for spastic cerebral palsy.Childs Nerv Syst. 2001 Jan;17(1-2):1-18. doi: 10.1007/pl00013722. Childs Nerv Syst. 2001. PMID: 11219613 Review.
Cited by
-
Combined intrathecal baclofen pump revision to the cervical level and lumbosacral ventral-dorsal rhizotomy for severe medically refractory hypertonia: illustrative cases.J Neurosurg Case Lessons. 2025 Jan 27;9(4):CASE24599. doi: 10.3171/CASE24599. Print 2025 Jan 27. J Neurosurg Case Lessons. 2025. PMID: 39869897 Free PMC article.
-
Muscle architecture, growth, and biological Remodelling in cerebral palsy: a narrative review.BMC Musculoskelet Disord. 2022 Mar 10;23(1):233. doi: 10.1186/s12891-022-05110-5. BMC Musculoskelet Disord. 2022. PMID: 35272643 Free PMC article. Review.
-
Novel ATL1 mutation in a Chinese family with hereditary spastic paraplegia: A case report and review of literature.World J Clin Cases. 2019 Jun 6;7(11):1358-1366. doi: 10.12998/wjcc.v7.i11.1358. World J Clin Cases. 2019. PMID: 31236401 Free PMC article.
-
Treatment of pediatric spasticity, including children with cerebral palsy, with Botox (onabotulinumtoxinA): Development, insights, and impact.Medicine (Baltimore). 2023 Jul 1;102(S1):e32363. doi: 10.1097/MD.0000000000032363. Medicine (Baltimore). 2023. PMID: 37499087 Free PMC article.
-
Noninvasive Fetal RhD Blood Group Genotyping: A Health Technology Assessment.Ont Health Technol Assess Ser. 2020 Nov 2;20(15):1-160. eCollection 2020. Ont Health Technol Assess Ser. 2020. PMID: 33240456 Free PMC article. Review.
References
-
- Surveillance of Cerebral Palsy in Europe. Surveillance of cerebral palsy in Europe: a collaboration of cerebral palsy surveys and registers. Surveillance of Cerebral Palsy in Europe (SCPE). Dev Med Child Neurol. 2000; 42(12):816–24. - PubMed
-
- Centers for Disease Control and Prevention. Economic costs associated with mental retardation, cerebral palsy, hearing loss, and vision impairment—United States, 2003. MMWR Morb Mortal Wkly Rep. 2004; 53(3):57–9. - PubMed
-
- Hankins GD, Speer M. Defining the pathogenesis and pathophysiology of neonatal encephalopathy and cerebral palsy. Obstet Gynecol. 2003; 102(3):628–36. - PubMed
-
- Rosenbaum P, Paneth N, Leviton A, Goldstein M, Bax M, Damiano D, et al. A report: the definition and classification of cerebral palsy April 2006. Dev Med Child Neurol Suppl. 2007; 109: 8–14. - PubMed
-
- Oskoui M, Coutinho F, Dykeman J, Jette N, Pringsheim T. An update on the prevalence of cerebral palsy: a systematic review and meta-analysis. Dev Med Child Neurol. 2013; 55(6):509–19. - PubMed