

Lung-Protective Ventilation Strategies for Relief from Ventilator-Associated Lung Injury in Patients Undergoing Craniotomy: A Bicenter Randomized, Parallel, and Controlled Trial
- PMID: 28757912
- PMCID: PMC5516714
- DOI: 10.1155/2017/6501248
Lung-Protective Ventilation Strategies for Relief from Ventilator-Associated Lung Injury in Patients Undergoing Craniotomy: A Bicenter Randomized, Parallel, and Controlled Trial
Abstract
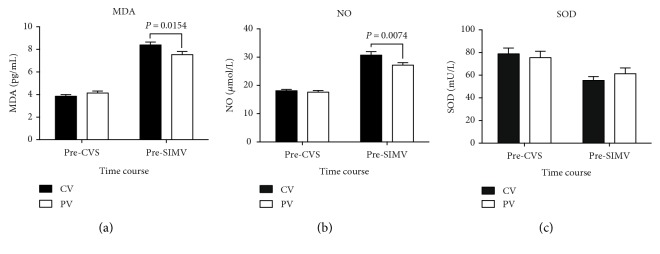
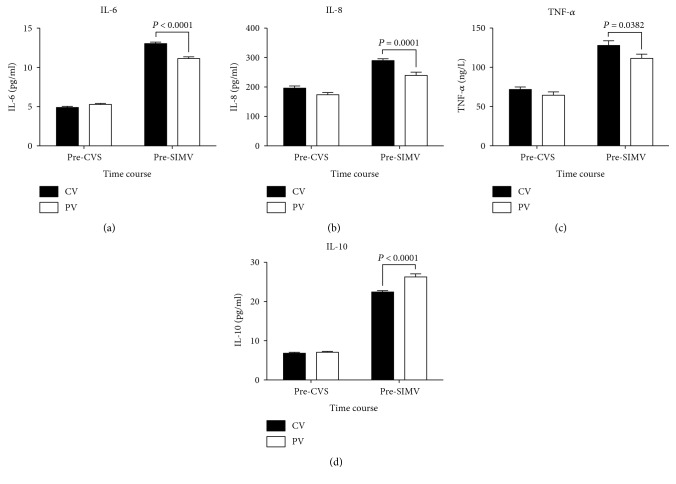
Current evidence indicates that conventional mechanical ventilation often leads to lung inflammatory response and oxidative stress, while lung-protective ventilation (LPV) minimizes the risk of ventilator-associated lung injury (VALI). This study evaluated the effects of LPV on relief of pulmonary injury, inflammatory response, and oxidative stress among patients undergoing craniotomy. Sixty patients undergoing craniotomy received either conventional mechanical (12 mL/kg tidal volume [VT] and 0 cm H2O positive end-expiratory pressure [PEEP]; CV group) or protective lung (6 mL/kg VT and 10 cm H2O PEEP; PV group) ventilation. Hemodynamic variables, lung function indexes, and inflammatory and oxidative stress markers were assessed. The PV group exhibited greater dynamic lung compliance and lower respiratory index than the CV group during surgery (P < 0.05). The PV group exhibited higher plasma interleukin- (IL-) 10 levels and lower plasma malondialdehyde and nitric oxide and bronchoalveolar lavage fluid, IL-6, IL-8, tumor necrosis factor-α, IL-10, malondialdehyde, nitric oxide, and superoxide dismutase levels (P < 0.05) than the CV group. There were no significant differences in hemodynamic variables, blood loss, liquid input, urine output, or duration of mechanical ventilation between the two groups (P > 0.05). Patients receiving LPV during craniotomy exhibited low perioperative inflammatory response, oxidative stress, and VALI.
Figures





Similar articles
-
The impact of tidal volume on pulmonary complications following minimally invasive esophagectomy: a randomized and controlled study.J Thorac Cardiovasc Surg. 2013 Nov;146(5):1267-73; discussion 1273-4. doi: 10.1016/j.jtcvs.2013.06.043. Epub 2013 Aug 28. J Thorac Cardiovasc Surg. 2013. PMID: 23993028 Clinical Trial.
-
Effects of different ventilation strategies on exhaled nitric oxide in geriatric abdominal surgery.J Breath Res. 2015 Feb 26;9(1):016006. doi: 10.1088/1752-7155/9/1/016006. J Breath Res. 2015. PMID: 25719610 Clinical Trial.
-
Low tidal volume and high positive end-expiratory pressure mechanical ventilation results in increased inflammation and ventilator-associated lung injury in normal lungs.Anesth Analg. 2010 Jun 1;110(6):1652-60. doi: 10.1213/ANE.0b013e3181cfc416. Epub 2010 Jan 26. Anesth Analg. 2010. PMID: 20103541
-
Advances in ventilator-associated lung injury: prevention is the target.Expert Rev Respir Med. 2014 Apr;8(2):233-48. doi: 10.1586/17476348.2014.890519. Expert Rev Respir Med. 2014. PMID: 24601663 Review.
-
Strategies to reduce ventilator-associated lung injury (VALI).Burns. 2013 Mar;39(2):200-11. doi: 10.1016/j.burns.2012.10.013. Epub 2012 Nov 24. Burns. 2013. PMID: 23183376 Review.
Cited by
-
Intraoperative use of low volume ventilation to decrease postoperative mortality, mechanical ventilation, lengths of stay and lung injury in adults without acute lung injury.Cochrane Database Syst Rev. 2018 Jul 9;7(7):CD011151. doi: 10.1002/14651858.CD011151.pub3. Cochrane Database Syst Rev. 2018. PMID: 29985541 Free PMC article.
-
PEEP application during mechanical ventilation contributes to fibrosis in the diaphragm.Respir Res. 2023 Feb 13;24(1):46. doi: 10.1186/s12931-023-02356-y. Respir Res. 2023. PMID: 36782202 Free PMC article.
-
Effect of flow-optimized pressure control ventilation-volume guaranteed (PCV-VG) on postoperative pulmonary complications: a consort study.J Cardiothorac Surg. 2024 Jul 8;19(1):425. doi: 10.1186/s13019-024-02881-x. J Cardiothorac Surg. 2024. PMID: 38978064 Free PMC article. Clinical Trial.
-
Dexmedetomidine with sufentanil in intravenous patient-controlled analgesia for relief from postoperative pain, inflammation and delirium after esophageal cancer surgery.Biosci Rep. 2020 May 29;40(5):BSR20193410. doi: 10.1042/BSR20193410. Biosci Rep. 2020. PMID: 32343308 Free PMC article. Clinical Trial.
-
Lung-protective ventilation worsens ventilator-induced diaphragm atrophy and weakness.Respir Res. 2020 Jan 10;21(1):16. doi: 10.1186/s12931-020-1276-7. Respir Res. 2020. PMID: 31924204 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
