

Pipeline embolization device retraction and foreshortening after internal carotid artery blister aneurysm treatment
- PMID: 28758549
- PMCID: PMC5814067
- DOI: 10.1177/1591019917722514
Pipeline embolization device retraction and foreshortening after internal carotid artery blister aneurysm treatment
Abstract
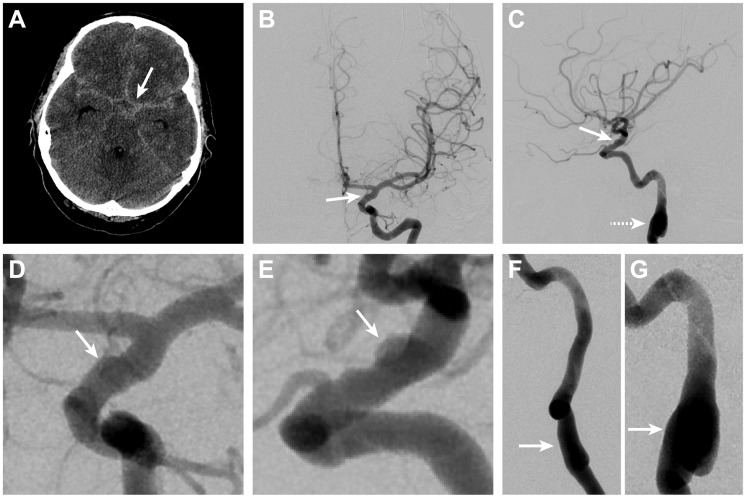
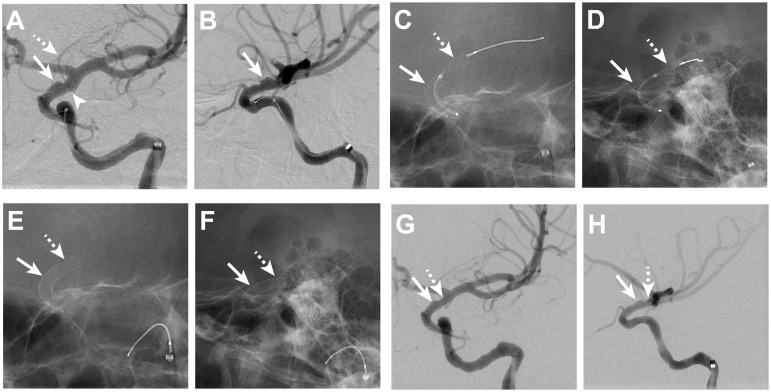
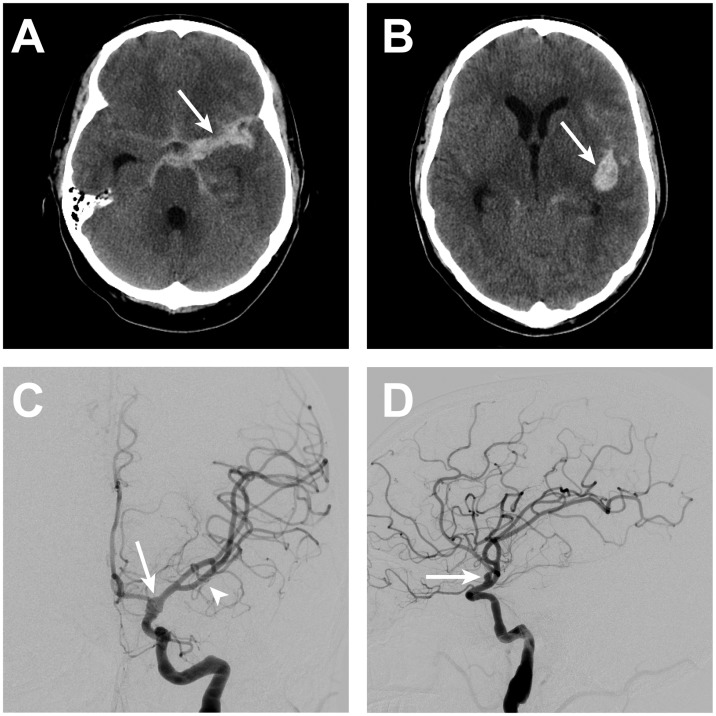
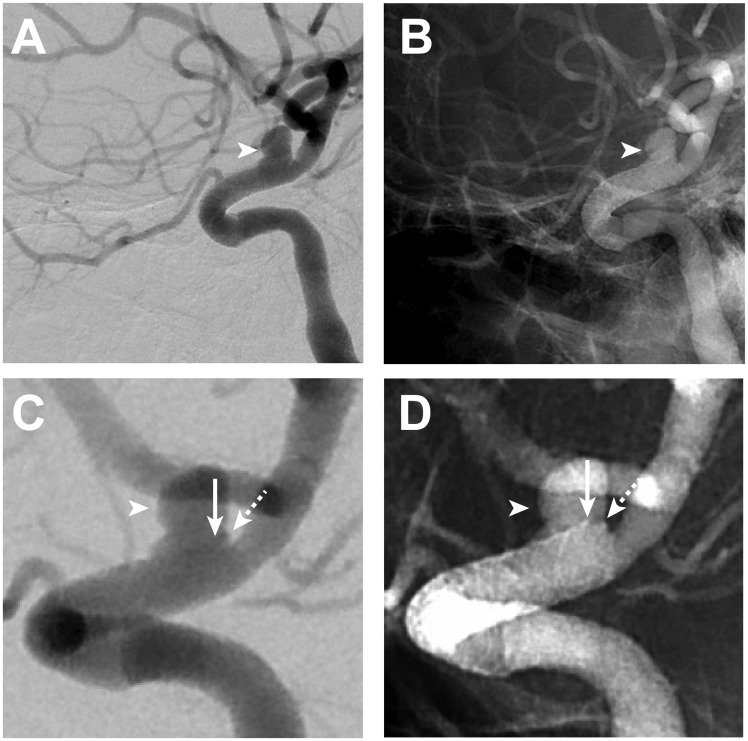
Background Subarachnoid hemorrhage (SAH) secondary to rupture of a blister aneurysm (BA) results in high morbidity and mortality. Endovascular treatment with the pipeline embolization device (PED) has been described as a new treatment strategy for these lesions. We present the first reported case of PED retraction and foreshortening after treatment of a ruptured internal carotid artery (ICA) BA. Case description A middle-aged patient presented with SAH secondary to ICA BA rupture. The patient was treated with telescoping PED placement across the BA. After 5 days from treatment, the patient developed a new SAH due to re-rupture of the BA. Digital subtraction angiography revealed an increase in caliber of the supraclinoid ICA with associated retraction and foreshortening of the PED that resulted in aneurysm uncovering and growth. Conclusions PED should be oversized during ruptured BA treatment to prevent device retraction and aneurysm regrowth. Frequent imaging follow up after BA treatment with PED is warranted to ensure aneurysm occlusion.
Keywords: Blister aneurysm; embolization; foreshortening; pipeline; subarachnoid hemorrhage.
Figures

References
-
- Szmuda T, Sloniewski P, Waszak PM, et al. Towards a new treatment paradigm for ruptured blood blister-like aneurysms of the internal carotid artery? A rapid systematic review. J Neurointerv Surg 2016; 8: 488–94. - PubMed
-
- Nerva JD, Morton RP, Levitt MR, et al. Pipeline embolization device as primary treatment for blister aneurysms and iatrogenic pseudoaneurysms of the internal carotid artery. J Neurointerv Surg 2015; 7: 210–216. - PubMed
-
- Linfante I, Mayich M, Sonig A, et al. Flow diversion with pipeline embolic device as treatment of subarachnoid hemorrhage secondary to blister aneurysms: Dual-center experience and review of the literature. J Neurointerv Surg 2017; 9: 29–33. - PubMed
-
- Hu YC, Chugh C, Mehta H, et al. Early angiographic occlusion of ruptured blister aneurysms of the internal carotid artery using the pipeline embolization device as a primary treatment option. J Neurointerv Surg 2014; 6: 740–743. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
