

EPA + DHA supplementation reduces PMN activation in microenvironment of chronic venous leg ulcers: A randomized, double-blind, controlled study
- PMID: 28758717
- PMCID: PMC9288800
- DOI: 10.1111/wrr.12558
EPA + DHA supplementation reduces PMN activation in microenvironment of chronic venous leg ulcers: A randomized, double-blind, controlled study
Abstract
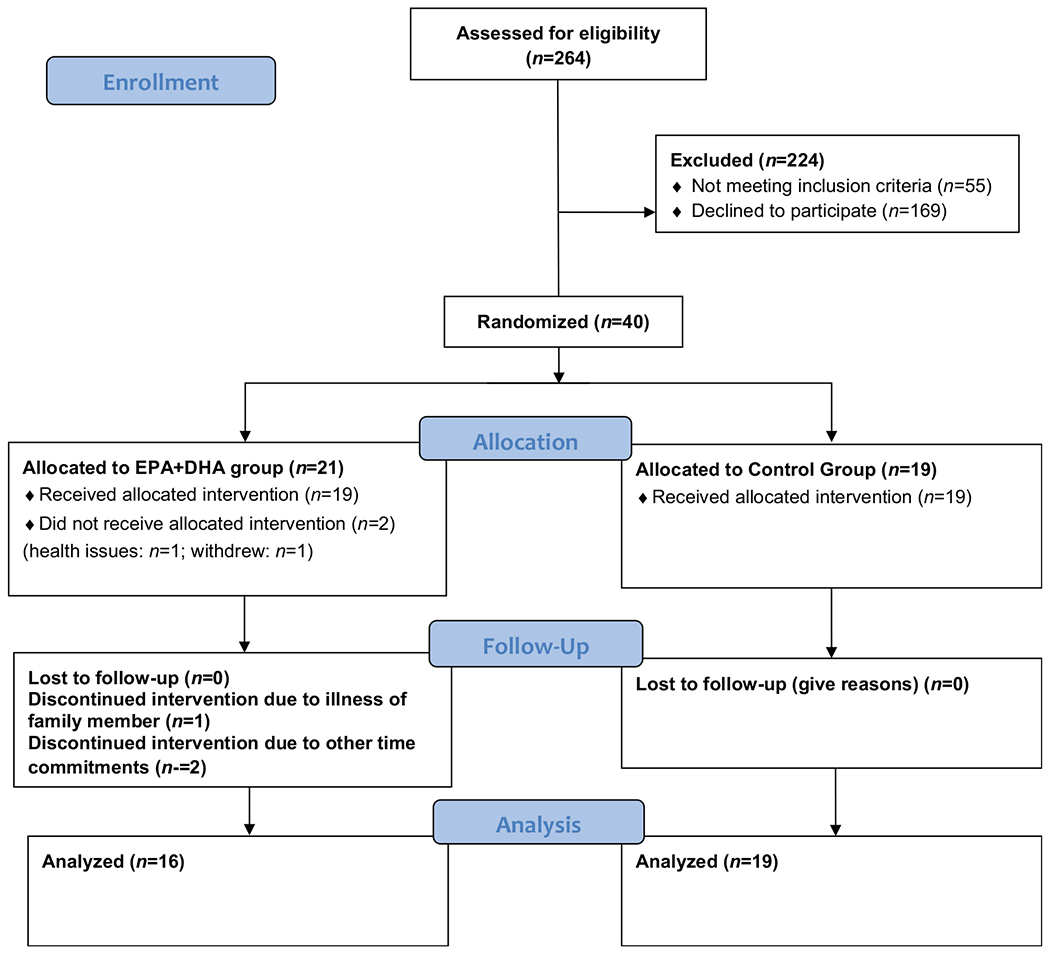
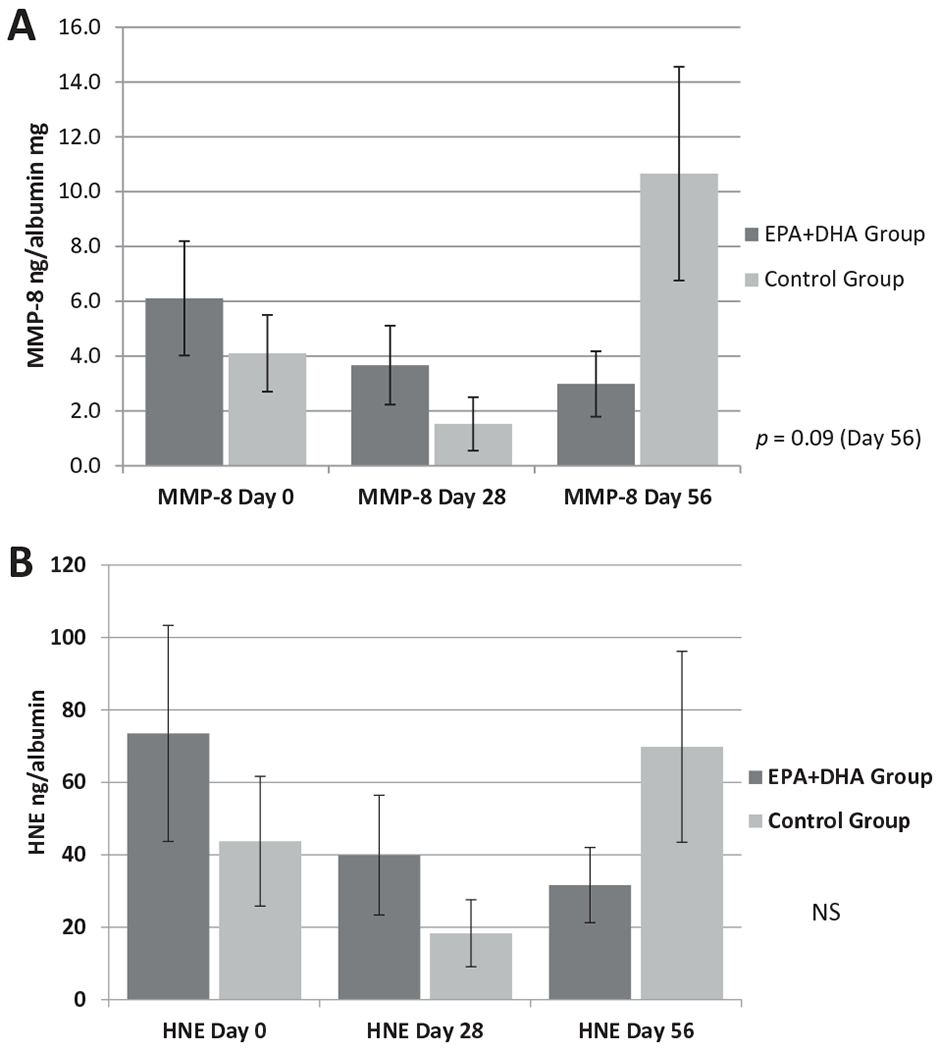
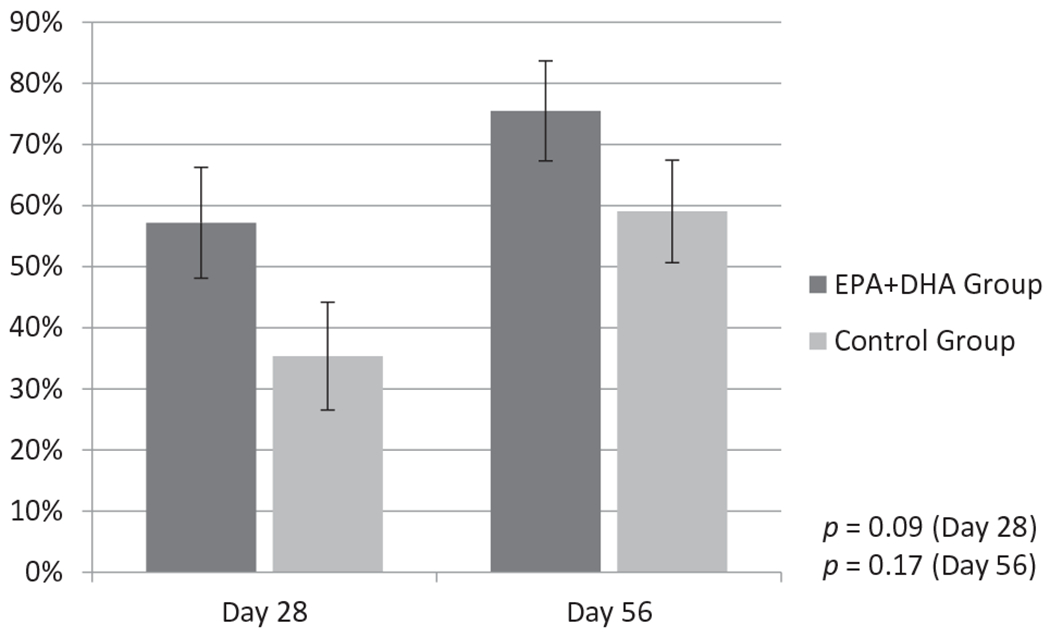
Sustained high levels of activated polymorphonuclear leukocytes (PMNs) and PMN-derived proteases in the microenvironment of chronic venous leg ulcers (CVLUs) are linked to chronic inflammation and delayed healing. Uncontrolled PMN activity eventually destroys newly developed tissue and degrades critical growth factors. The bioactive components of fish oil (n-3 eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) have strong inflammation-resolving actions and have been shown to assuage PMN activity, but have not been tested in CVLU patients. This randomized controlled study compared the effectiveness of oral EPA + DHA therapy to a placebo for reducing PMN activation in CVLU microenvironments. At Days 0, 28, and 56, markers of PMNs (CD15) and activated PMNs (CD66b), and levels of PMN-derived proteases human neutrophil elastase and matrix metalloproteinase-8 were measured in CVLU fluid from patients receiving standard compression therapy and (1) EPA + DHA therapy (n = 16) or (2) placebo (n = 19). By Day 56, the EPA + DHA Group had a significantly lower percentage of CD66b+ cells in CVLU fluid compared to Day 0 (p = 0.02) and to Day 28 (p = 0.05). Importantly, there were downward trends in levels of both matrix metalloproteinase-8 and human neutrophil elastase over time in the EPA + DHA Group, which also demonstrated greater reductions in wound area by Day 28 (57% reduction) and Day 56 (76% reduction) than the Control Group (35% and 59%, respectively). Moreover, reductions in wound area had significant negative relationships with CD15+ cells in wound fluid at Days 28 (p = 0.008) and 56 (p < 0.001), and CD66b+ cells at Days 28 (p = 0.04) and 56 (p = 0.009). The collective findings provide supplemental evidence that high levels of activated PMNs in CVLU microenvironments inhibit healing, and suggest that EPA + DHA oral therapy may modulate PMN activity and facilitate healing of CVLUs when added to standard care regimens.
© 2017 by the Wound Healing Society.
Conflict of interest statement
Figures
References
-
- Rice JB, Desai U, Cummings AK, Birnbaum HG, Skornicki M, Parsons N. Burden of venous leg ulcers in the United States. J Med Econ 2014; 17: 347–56. - PubMed
-
- Gould LJ, Dosi G, Couch K, Gibbons GW, Howell RS, Brem H, Tomic M. Modalities to treat venous ulcers: compression, surgery, and bioengineered tissue. Plast Reconstr Surg 2016; 138 (3 Suppl.): 199S–208S. - PubMed
-
- van Rij AM, De Alwis CS, Jiang P, Christie RA, Hill GB, Dutton SJ, Thomson IA. Obesity and impaired venous function. Eur J Vasc Endovasc Surg 2008; 35: 739–44. - PubMed
-
- Alavi A, Sibbald RG, Phillips TJ, Miller OF, Margolis DJ, Marston W, et al. What’s new: management of venous leg ulcers: treating venous leg ulcers. J Am Acad Dermatol 2016; 74: 643–64; quiz 665–64. - PubMed
-
- Margolis DJ, Bilker W, Santanna J, Baumgarten M. Venous leg ulcer: incidence and prevalence in the elderly. J Am Acad Dermatol 2002; 46: 381–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
