

Assessment of Bone Metastases in Patients with Prostate Cancer-A Comparison between 99mTc-Bone-Scintigraphy and [68Ga]Ga-PSMA PET/CT
- PMID: 28758969
- PMCID: PMC5620612
- DOI: 10.3390/ph10030068
Assessment of Bone Metastases in Patients with Prostate Cancer-A Comparison between 99mTc-Bone-Scintigraphy and [68Ga]Ga-PSMA PET/CT
Abstract
Purpose: Bone scintigraphy is the standard of reference in bone metastases in prostate cancer patients. However, new radiotracers employed in prostate-specific membrane antigen (PSMA)-ligands has led to the growing importance of PET/CT as diagnostic tool. The aim of our study was to investigate the difference between bone scan and PSMA-PET/CT for the detection of bone metastases in prostate cancer.
Methods: Thirty patients with bone metastases originating from prostate cancer were examined by 99mTc-MDP bone scan and 68Ga-PSMA-PET/CT within an average of 21 days. Bone scans were analyzed visually according to the number of lesions and using the software package ExiniBONE by Exini Diagnostics. PET/CT data was analyzed visually. Numbers of detected lesions were compared for the different methods for the whole patient and for different regions. In addition, results were compared to serum prostate-specific antigen (PSA), alkaline phosphatase (ALP), bone alkaline phosphatase (bALP), pro gastrin releasing peptide (pGRP) and eastern cooperative oncology group (ECOG) performance status.
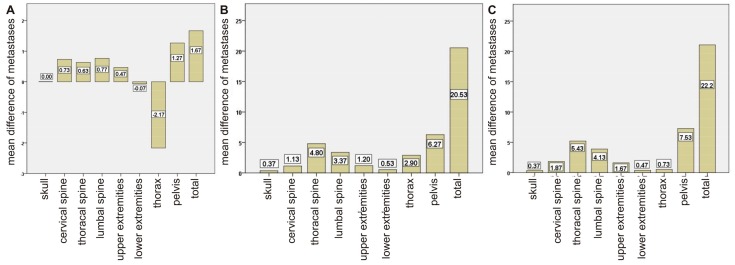
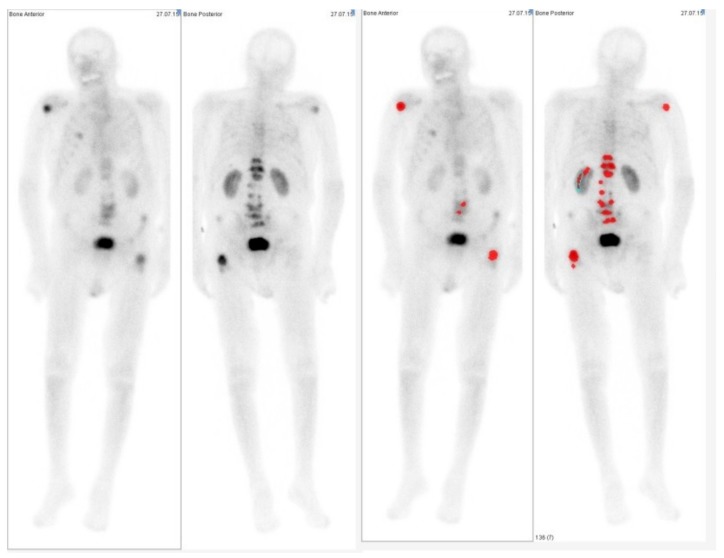
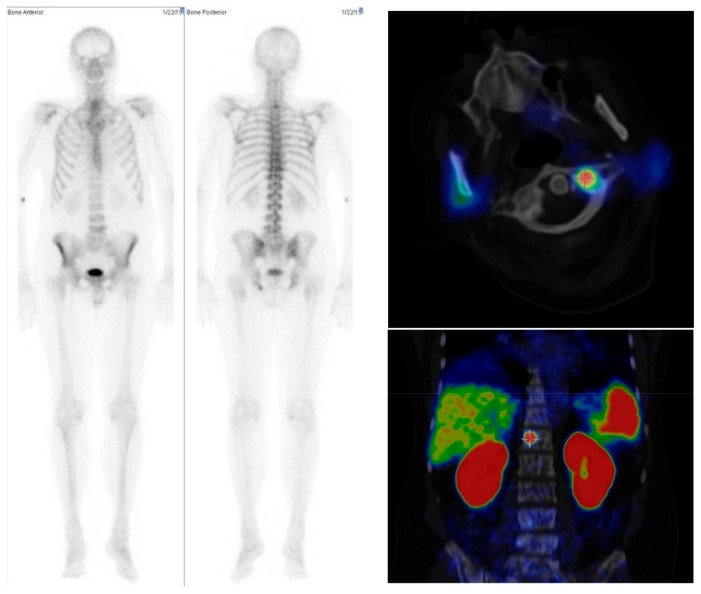
Results: In the bone scans, visual and semiautomatic lesion detection showed similar results with an average of 19.4 and 17.8 detected bone lesion per patient. However, in PSMA-PET/CT, on average double the numbers of lesions (40.0) were detected. The largest differences were found in the thorax and pelvis, which can be explained by the advantages of tomographic imaging. Bland-Altman analysis showed greater differences in patients with large numbers of bone metastases.
Conclusion: No significant difference was found when using semiautomatic analysis compared to visual reading for bone scans. Fewer bone metastases were detected in bone scans than in PSMA-PET/CT. However, in none of our patients would the difference have led to clinical consequences. Therefore, it seems that for patients undergoing PSMA-PET/CT, there is no need to perform additional bone scans if the appropriate PET/CT protocols are applied.
Keywords: PSMA-PET/CT; bone scan index; bone scintigraphy; prostate cancer.
Conflict of interest statement
The EXINI boneBSI software was provided for free in context of a non-commercial research agreement between R.A.B. and EXINI Diagnostics. R.A.B. and M.E. are consultants to Bayer Healthcare AG (Leverkusen, Germany), L.T. received travelling support from Bayer Healthcare AG (Leverkusen, Germany), R.A.B. is in the speakers bureau of Mediso Medical Imaging Systems Ltd. (Budapest, Hungary). All other authors had full control of the data and information submitted for publication. No potential conflicts of interest were disclosed by the other authors.
Figures

References
-
- Surveillance, Epidemiology, and End Results Program . In: SEER Stat Fact Sheets: Prostate Cancer. Site NCIW, editor. Surveillance, Epidemiology, and End Results Program; Rockville, MD, USA: 2015.
-
- Heidenreich A., Bastian P.J., Bellmunt J., Bolla M., Joniau S., van der Kwast T., Mason M., Matveev V., Wiegel T., Zattoni F., et al. EAU guidelines on prostate cancer. Part 1: Screening, diagnosis, and local treatment with curative intent-update 2013. Eur. Urol. 2014;65:124–137. doi: 10.1016/j.eururo.2013.09.046. - DOI - PubMed
-
- Imbriaco M., Larson S.M., Yeung H.W., Mawlawi O.R., Erdi Y., Venkatraman E.S., Scher H.I. A new parameter for measuring metastatic bone involvement by prostate cancer: The bone scan index. Clin. Cancer Res. 1998;4:1765–1772. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
