

Elevated Soluble Urokinase Plasminogen Activator Receptor and Proenkephalin Serum Levels Predict the Development of Acute Kidney Injury after Cardiac Surgery
- PMID: 28758975
- PMCID: PMC5578052
- DOI: 10.3390/ijms18081662
Elevated Soluble Urokinase Plasminogen Activator Receptor and Proenkephalin Serum Levels Predict the Development of Acute Kidney Injury after Cardiac Surgery
Abstract
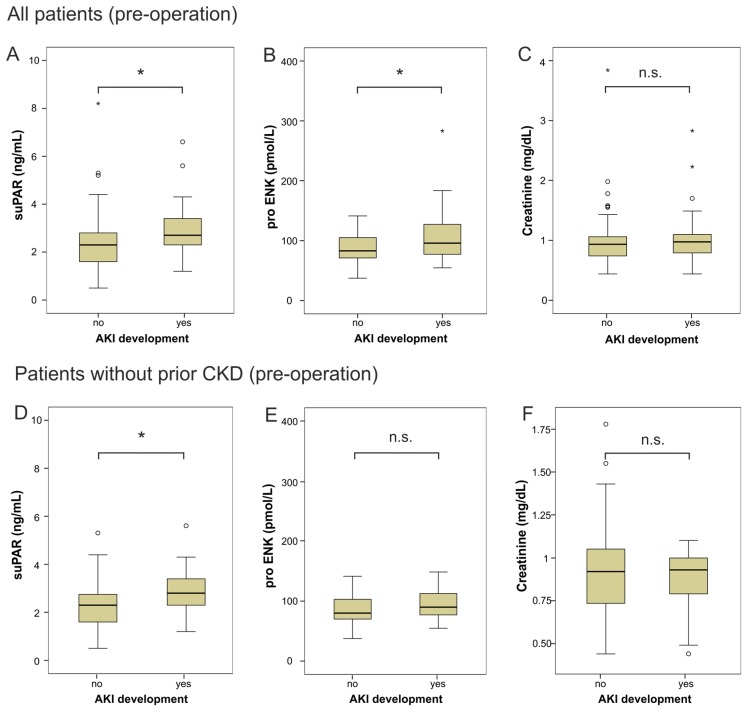
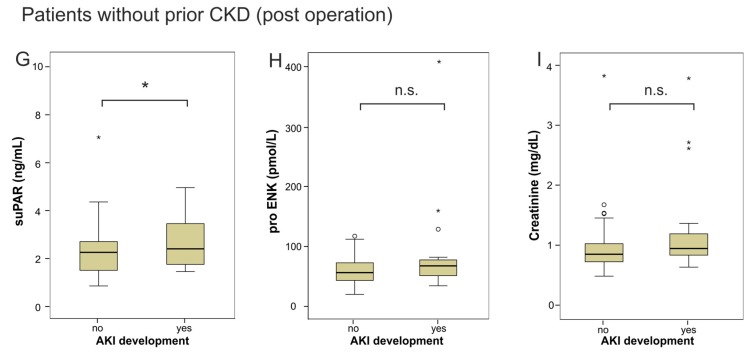
Acute kidney injury (AKI) develops in up to 40% of patients after cardiac surgery. The soluble urokinase plasminogen activator receptor (suPAR) has been identified as a biomarker for incident chronic kidney disease (CKD). Proenkephalin (proENK) also has been shown to be a biomarker for renal dysfunction. We hypothesized that pre-surgery suPAR and proENK levels might predict AKI in patients undergoing cardiac surgery. Consecutive patients (n = 107) undergoing elective cardiac surgery were studied prospectively. Clinical data, laboratory parameters, suPAR and proENK serum levels were assessed before operation, after operation and days one and four post-operatively. A total of 21 (19.6%) patients developed AKI within the first four days after elective surgery. Serum levels of suPAR and proENK, but not of creatinine, were significantly higher before surgery in these patients compared to those patients without AKI. This difference remained significant for suPAR, if patients with or without AKI were matched for risk factors (hypertension, diabetes, CKD). If cardiac surgery patients with pre-existing CKD (n = 10) were excluded, only pre-operative suPAR but not proENK serum levels remained significantly elevated in patients with subsequent AKI. Thus, our findings indicate that suPAR may be a predictive biomarker for AKI in the context of cardiac surgery, even in patients without underlying CKD.
Keywords: acute kidney failure; acute kidney injury; biomarker; cardiac surgery; pro-ENK; proenkephalin; soluble urokinase plasminogen activator receptor; suPAR.
Conflict of interest statement
Joachim Struck is an employee of Sphingotec GmbH (Hennigsdorf, Germany). The measurement of proenkephalin levels were performed blinded by Sphingotec GmbH. SuPAR assays were kindly provided by Virogates (Birkerød, Denmark).
Figures
References
-
- Brown J.R., Cochran R.P., Dacey L.J., Ross C.S., Kunzelman K.S., Dunton R.F., Braxton J.H., Charlesworth D.C., Clough R.A., Helm R.E., et al. Perioperative increases in serum creatinine are predictive of increased 90-day mortality after coronary artery bypass graft surgery. Circulation. 2006;114(Suppl. 1):1409–1413. doi: 10.1161/CIRCULATIONAHA.105.000596. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
