

A web-based tool to predict acute kidney injury in patients with ST-elevation myocardial infarction: Development, internal validation and comparison
- PMID: 28759604
- PMCID: PMC5536350
- DOI: 10.1371/journal.pone.0181658
A web-based tool to predict acute kidney injury in patients with ST-elevation myocardial infarction: Development, internal validation and comparison
Abstract
Background: In ST-elevation myocardial infarction (STEMI), acute kidney injury (AKI) may increase subsequent morbidity and mortality. Still, it remains difficult to predict AKI risk in these patients. We sought to 1) determine the frequency and clinical outcomes of AKI and, 2) develop, validate and compare a web-based tool for predicting AKI.
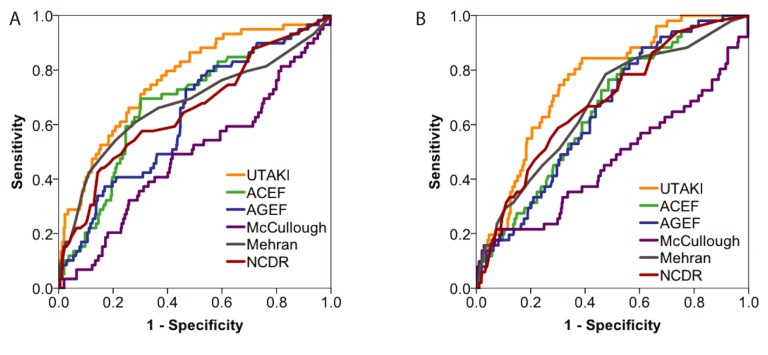
Methods & findings: In a racially diverse series of 1144 consecutive STEMI patients, Stage 1 or greater AKI occurred in 12.9% and was severe (Stage 2-3) in 2.9%. AKI was associated with increased mortality (5.7-fold, unadjusted) and hospital stay (2.5-fold). AKI was associated with systolic dysfunction, increased left ventricular end-diastolic pressures, hypotension and intra-aortic balloon counterpulsation. A computational algorithm (UT-AKI) was derived and internally validated. It showed higher sensitivity and improved overall prediction for AKI (area under the curve 0.76) vs. other published indices. Higher UT-AKI scores were associated with more severe AKI, longer hospital stay and greater hospital mortality.
Conclusions: In a large, racially diverse cohort of STEMI patients, Stage 1 or greater AKI was relatively common and was associated with significant morbidity and mortality. A web-accessible, internally validated tool was developed with improved overall value for predicting AKI. By identifying patients at increased risk, this tool may help physicians tailor post-procedural diagnostic and therapeutic strategies after STEMI to reduce AKI and its associated morbidity and mortality.
Conflict of interest statement
Figures

References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–128. doi: 10.1016/S0140-6736(12)61728-0 . - DOI - PMC - PubMed
-
- Maeder M, Klein M, Fehr T, Rickli H. Contrast nephropathy: review focusing on prevention. J Am Coll Cardiol. 2004;44(9):1763–71. Epub 2004/11/03. S0735-1097(04)01613-4 [pii] doi: 10.1016/j.jacc.2004.06.075 . - DOI - PubMed
-
- Mangano CM, Diamondstone LS, Ramsay JG, Aggarwal A, Herskowitz A, Mangano DT. Renal Dysfunction after Myocardial Revascularization: Risk Factors, Adverse Outcomes, and Hospital Resource Utilization. Annals of Internal Medicine. 1998;128(3):194–203. doi: 10.7326/0003-4819-128-3-199802010-00005 - DOI - PubMed
-
- Marenzi G, Assanelli E, Campodonico J, Lauri G, Marana I, De Metrio M, et al. Contrast Volume During Primary Percutaneous Coronary Intervention and Subsequent Contrast-Induced Nephropathy and Mortality. Annals of Internal Medicine. 2009;150(3):170–7. doi: 10.7326/0003-4819-150-3-200902030-00006 - DOI - PubMed
-
- Ranucci M, Castelvecchio S, Menicanti L, Frigiola A, Pelissero G. Risk of Assessing Mortality Risk in Elective Cardiac Operations: Age, Creatinine, Ejection Fraction, and the Law of Parsimony. Circulation. 2009;119(24):3053–61. doi: 10.1161/CIRCULATIONAHA.108.842393 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
