

Spatial modelling of contribution of individual level risk factors for mortality from Middle East respiratory syndrome coronavirus in the Arabian Peninsula
- PMID: 28759623
- PMCID: PMC5536289
- DOI: 10.1371/journal.pone.0181215
Spatial modelling of contribution of individual level risk factors for mortality from Middle East respiratory syndrome coronavirus in the Arabian Peninsula
Abstract
Background: Middle East respiratory syndrome coronavirus is a contagious respiratory pathogen that is contracted via close contact with an infected subject. Transmission of the pathogen has occurred through animal-to-human contact at first followed by human-to-human contact within families and health care facilities.
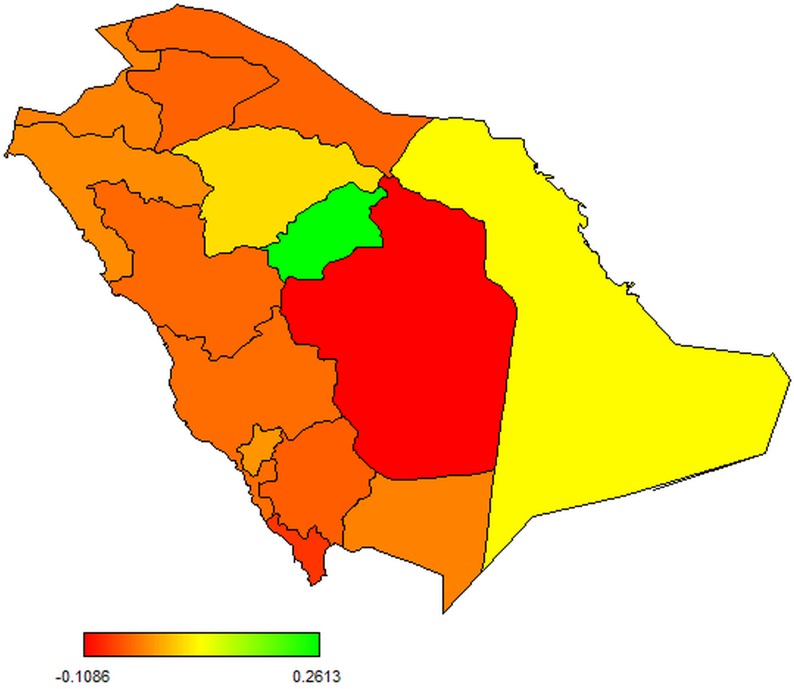
Data and methods: This study is based on a retrospective analysis of the Middle East respiratory syndrome coronavirus outbreak in the Kingdom of Saudi Arabia between June 2012 and July 2015. A Geoadditive variable model for binary outcomes was applied to account for both individual level risk factors as well spatial variation via a fully Bayesian approach.
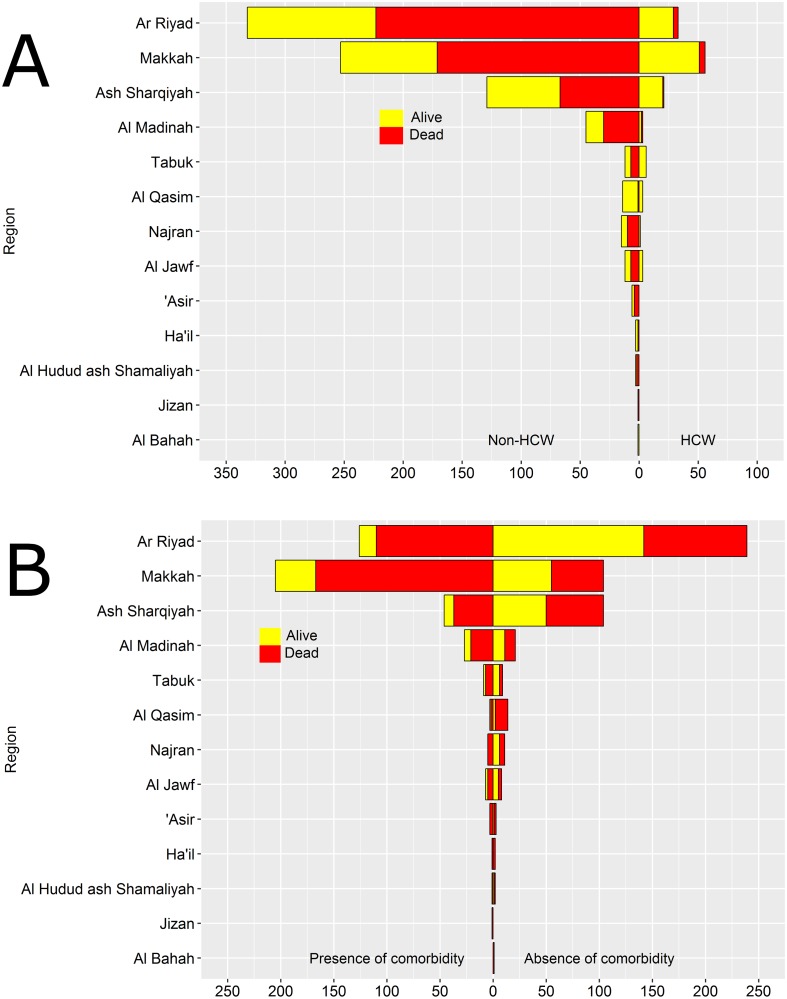
Results: Out of 959 confirmed cases, 642 (67%) were males and 317 (33%) had died. Three hundred and sixty four (38%) cases occurred in Ar Riyad province, while 325 (34%) cases occurred in Makkah. Individuals with some comorbidity had a significantly higher likelihood of dying from MERS-CoV compared with those who did not suffer comorbidity [Odds ratio (OR) = 2.071; 95% confidence interval (CI): 1.307, 3.263]. Health-care workers were significantly less likely to die from the disease compared with non-health workers [OR = 0.372, 95% CI: 0.151, 0.827]. Patients who had fatal clinical experience and those with clinical and subclinical experiences were equally less likely to die from the disease compared with patients who did not have fatal clinical experience and those without clinical and subclinical experiences respectively. The odds of dying from the disease was found to increase as age increased beyond 25 years and was much higher for individuals with any underlying comorbidities.
Conclusion: Interventions to minimize mortality from the Middle East respiratory syndrome coronavirus should particularly focus individuals with comorbidity, non-health-care workers, patients with no clinical fatal experience, and patients without any clinical and subclinical experiences.
Conflict of interest statement
Figures


References
-
- Cauchemez S, Van Kerkhove M, Riley S, Donnelly C, Fraser C, Ferguson N. Transmission scenarios for Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and how to tell them apart. Euro surveillance: bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin. 2013;18(24). - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
