

Early-Life Epilepsies and the Emerging Role of Genetic Testing
- PMID: 28759667
- PMCID: PMC5710404
- DOI: 10.1001/jamapediatrics.2017.1743
Early-Life Epilepsies and the Emerging Role of Genetic Testing
Abstract
Importance: Early-life epilepsies are often a consequence of numerous neurodevelopmental disorders, most of which are proving to have genetic origins. The role of genetic testing in the initial evaluation of these epilepsies is not established.
Objective: To provide a contemporary account of the patterns of use and diagnostic yield of genetic testing for early-life epilepsies.
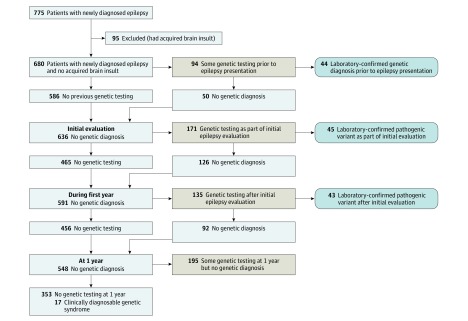
Design, setting, and participants: In this prospective cohort, children with newly diagnosed epilepsy with an onset at less than 3 years of age were recruited from March 1, 2012, to April 30, 2015, from 17 US pediatric hospitals and followed up for 1 year. Of 795 families approached, 775 agreed to participate. Clinical diagnosis of the etiology of epilepsy were characterized based on information available before genetic testing was performed. Added contributions of cytogenetic and gene sequencing investigations were determined.
Exposures: Genetic diagnostic testing.
Main outcomes and measures: Laboratory-confirmed pathogenic variant.
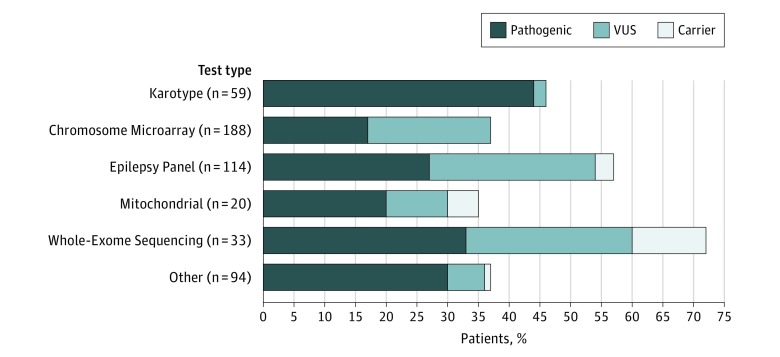
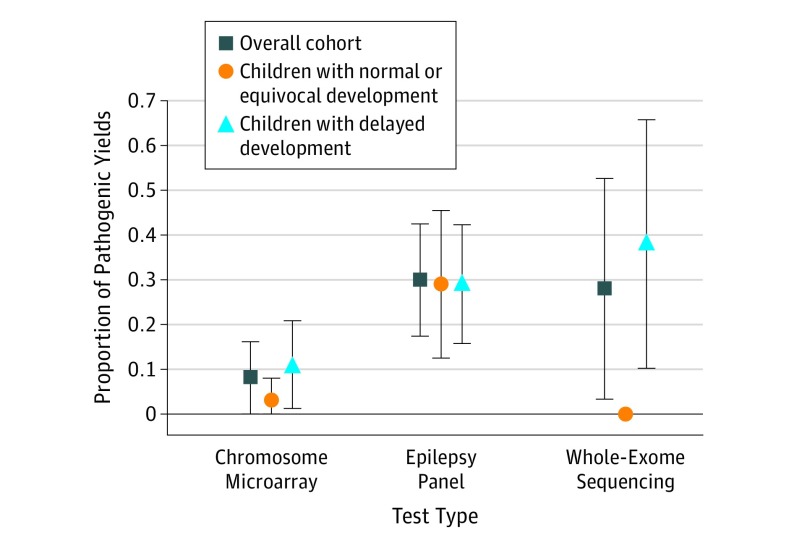
Results: Of the 775 patients in the study (367 girls and 408 boys; median age of onset, 7.5 months [interquartile range, 4.2-16.5 months]), 95 (12.3%) had acquired brain injuries. Of the remaining 680 patients, 327 (48.1%) underwent various forms of genetic testing, which identified pathogenic variants in 132 of 327 children (40.4%; 95% CI, 37%-44%): 26 of 59 (44.1%) with karyotyping, 32 of 188 (17.0%) with microarrays, 31 of 114 (27.2%) with epilepsy panels, 11 of 33 (33.3%) with whole exomes, 4 of 20 (20.0%) with mitochondrial panels, and 28 of 94 (29.8%) with other tests. Forty-four variants were identified before initial epilepsy presentation. Apart from dysmorphic syndromes, pathogenic yields were highest for children with tuberous sclerosis complex (9 of 11 [81.8%]), metabolic diseases (11 of 14 [78.6%]), and brain malformations (20 of 61 [32.8%]). A total of 180 of 446 children (40.4%), whose etiology would have remained unknown without genetic testing, underwent some testing. Pathogenic variants were identified in 48 of 180 children (26.7%; 95% CI, 18%-34%). Diagnostic yields were greater than 15% regardless of delay, spasms, and young age. Yields were greater for epilepsy panels (28 of 96 [29.2%]; P < .001) and whole exomes (5 of 18 [27.8%]; P = .02) than for chromosomal microarray (8 of 101 [7.9%]).
Conclusions and relevance: Genetic investigations, particularly broad sequencing methods, have high diagnostic yields in newly diagnosed early-life epilepsies regardless of key clinical features. Thorough genetic investigation emphasizing sequencing tests should be incorporated into the initial evaluation of newly presenting early-life epilepsies and not just reserved for those with severe presentations and poor outcomes.
Conflict of interest statement
Figures
Comment in
-
Two Studies, One Message: High Yield of Genetic Testing in Infants and Young Children With Severe Epilepsies.Epilepsy Curr. 2018 Jan-Feb;18(1):24-26. doi: 10.5698/1535-7597.18.1.24. Epilepsy Curr. 2018. PMID: 29844755 Free PMC article. No abstract available.
-
Updates for Child Neurology.Pediatr Ann. 2021 Jun;50(6):e240-e241. doi: 10.3928/19382359-20210517-02. Epub 2021 Jun 1. Pediatr Ann. 2021. PMID: 34115561 No abstract available.
References
-
- Camfield CS, Camfield PR, Gordon K, Wirrell E, Dooley JM. Incidence of epilepsy in childhood and adolescence: a population-based study in Nova Scotia from 1977 to 1985. Epilepsia. 1996;37(1):19-23. - PubMed
-
- Commission on Classification and Terminology of the International League Against Epilepsy Proposal for revised classification of epilepsies and epileptic syndromes. Epilepsia. 1989;30(4):389-399. - PubMed
-
- Camfield C, Camfield P. Twenty years after childhood-onset symptomatic generalized epilepsy the social outcome is usually dependency or death: a population-based study. Dev Med Child Neurol. 2008;50(11):859-863. - PubMed
-
- Glauser TA. Topiramate in the catastrophic epilepsies of childhood. J Child Neurol. 2000;15(suppl 1):S14-S21. - PubMed
-
- Glauser TA. Following catastrophic epilepsy patients from childhood to adulthood. Epilepsia. 2004;45(suppl 5):23-26. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
