

Surgical treatment of large and giant cavernous carotid aneurysms
- PMID: 28761512
- PMCID: PMC5532919
- DOI: 10.4103/1793-5482.180930
Surgical treatment of large and giant cavernous carotid aneurysms
Abstract
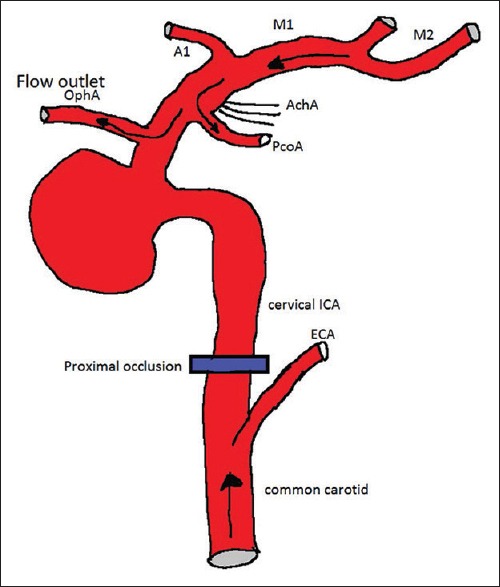
Cavernous carotid aneurysms (CCAs) are uncommon pathologic entities. Extradural place and the skull base location make this type of an aneurysm different in clinical features and treatment techniques. Direct aneurysm clipping is technically difficult and results in a significant postoperative neurological deficit. Therefore, several techniques of indirect surgical treatment were developed with different surgical outcomes, such as proximal occlusion of internal carotid artery (ICA) or trapping with or without bypass (superficial temporal artery-middle cerebral artery bypass or high-flow bypass). High-flow bypass with proximal ICA occlusion seems to be the most appropriate surgical treatment for CCA because of the high rate of symptom improvement, aneurysm thrombosis, and minimal postoperative complications. However, in cases of CCA presented with direct carotid-cavernous fistula, the appropriate surgical treatment is high-flow bypass with aneurysm trapping, which the fistula can be obliterated immediately after surgery.
Keywords: Cavernous carotid aneurysm; giant aneurysm; high-flow bypass; intracavernous carotid aneurysm; large aneurysm; proximal occlusion; surgical treatment; trapping.
Conflict of interest statement
There are no conflicts of interest.
Figures





Similar articles
-
Surgical Trapping of a Cavernous Carotid Aneurysm Causing Carotid Cavernous Fistula After Flow Diverter Placement: Technical Note and Literature Review.World Neurosurg. 2023 Sep;177:31-38. doi: 10.1016/j.wneu.2023.05.095. Epub 2023 Jun 1. World Neurosurg. 2023. PMID: 37268190
-
Combining Internal Carotid Ligation with Low-Flow Bypass for Treating Large-Giant Cavernous Sinus Segment Aneurysms: A Report of Four Cases.World Neurosurg. 2017 Apr;100:280-287. doi: 10.1016/j.wneu.2017.01.011. Epub 2017 Jan 16. World Neurosurg. 2017. PMID: 28093349
-
Urgent treatment of severe symptomatic direct carotid cavernous fistula caused by ruptured cavernous internal carotid artery aneurysm using high-flow bypass, proximal ligation, and direct distal clipping: Technical case report.Surg Neurol Int. 2014 Apr 15;5:49. doi: 10.4103/2152-7806.130772. eCollection 2014. Surg Neurol Int. 2014. PMID: 24818056 Free PMC article.
-
Bilateral cavernous carotid aneurysms treated by two-stage extracranial-intracranial bypass followed by parent artery occlusion: case report and literature review.Acta Neurochir (Wien). 2017 Sep;159(9):1693-1698. doi: 10.1007/s00701-017-3101-8. Epub 2017 Feb 8. Acta Neurochir (Wien). 2017. PMID: 28181086 Review.
-
Massive Epistaxis from Nontraumatic Cavernous Carotid Aneurysm Treated by High-Flow Bypass and Cervical Internal Carotid Artery Ligation: A Case Report and Review of the Literature.World Neurosurg. 2019 Aug;128:23-28. doi: 10.1016/j.wneu.2019.04.213. Epub 2019 May 1. World Neurosurg. 2019. PMID: 31054341 Review.
Cited by
-
Bilateral blindness following flow diverter placement in a giant thrombosed cavernous carotid aneurysm: illustrative case.J Neurosurg Case Lessons. 2022 Dec 12;4(24):CASE22352. doi: 10.3171/CASE22352. Print 2022 Dec 12. J Neurosurg Case Lessons. 2022. PMID: 36681971 Free PMC article.
-
Concomitant occurrence of clinoid and cavernous segment aneurysms complicated with carotid cavernous fistula: A case report.Medicine (Baltimore). 2019 Nov;98(48):e18184. doi: 10.1097/MD.0000000000018184. Medicine (Baltimore). 2019. PMID: 31770272 Free PMC article.
-
Spontaneous thrombosis of a giant cavernous-carotid aneurysm with simultaneous ipsilateral complete parent artery occlusion: a rare phenomenon and review of the literature.Arch Clin Cases. 2023 Feb 20;10(1):21-28. doi: 10.22551/2023.38.1001.10234. eCollection 2023. Arch Clin Cases. 2023. PMID: 36814678 Free PMC article.
-
High-Flow Bypass with Radial Artery Graft for Cavernous Carotid Aneurysms: A Case Series.Asian J Neurosurg. 2020 Dec 21;15(4):863-869. doi: 10.4103/ajns.AJNS_289_20. eCollection 2020 Oct-Dec. Asian J Neurosurg. 2020. PMID: 33708655 Free PMC article.
-
Microsurgical partial trapping for the treatment of unclippable vertebral artery aneurysms: Experience from 27 patients and review of literature.World Neurosurg X. 2023 Dec 5;21:100256. doi: 10.1016/j.wnsx.2023.100256. eCollection 2024 Jan. World Neurosurg X. 2023. PMID: 38163051 Free PMC article.
References
-
- Mikabe T, Ogihara R, Tomita S, Kin H, Karasawa H, Watanabe S, et al. Giant intracranial aneurysm visualized by prolonged injection angiography – Case report (author's transl) No Shinkei Geka. 1980;8:749–53. - PubMed
-
- Russell SM, Jafar JJ. Microsurgical treatment of intracavernous carotid artery aneurysms. In: Le Roux PD, Winn RH, Newell DW, editors. Management of Cerebral Aneurysms. Philadelphia: Saunders; 2004. pp. 711–29.
-
- Hahn CD, Nicolle DA, Lownie SP, Drake CG. Giant cavernous carotid aneurysms: Clinical presentation in fifty-seven cases. J Neuroophthalmol. 2000;20:253–8. - PubMed
-
- Silva MN, Saeki N, Hirai S, Yamaura A. Unusual cranial nerve palsy caused by cavernous sinus aneurysms. Clinical and anatomical considerations reviewed. Surg Neurol. 1999;52:143–8. - PubMed
-
- Whittle IR, Williams DB, Halmagyi GM, Besser M. Spontaneous thrombosis of a giant intracranial aneurysm and ipsilateral internal carotid artery. Case report. J Neurosurg. 1982;56:287–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous