

Endoscopic Stenting as Bridge to Surgery versus Emergency Resection for Left-Sided Malignant Colorectal Obstruction: An Updated Meta-Analysis
- PMID: 28761765
- PMCID: PMC5516723
- DOI: 10.1155/2017/2863272
Endoscopic Stenting as Bridge to Surgery versus Emergency Resection for Left-Sided Malignant Colorectal Obstruction: An Updated Meta-Analysis
Abstract
Introduction: Emergency resection represents the traditional treatment for left-sided malignant obstruction. However, the placement of self-expanding metallic stents and delayed surgery has been proposed as an alternative approach. The aim of the current meta-analysis was to review the available evidence, with particular interest for the short-term outcomes, including a recent multicentre RCT.
Methods: We considered randomized controlled trials comparing stenting as a bridge to surgery and emergency surgery for the management of left-sided malignant large bowel obstruction, performing a systematic review in MEDLINE, PubMed database, and the Cochrane libraries.
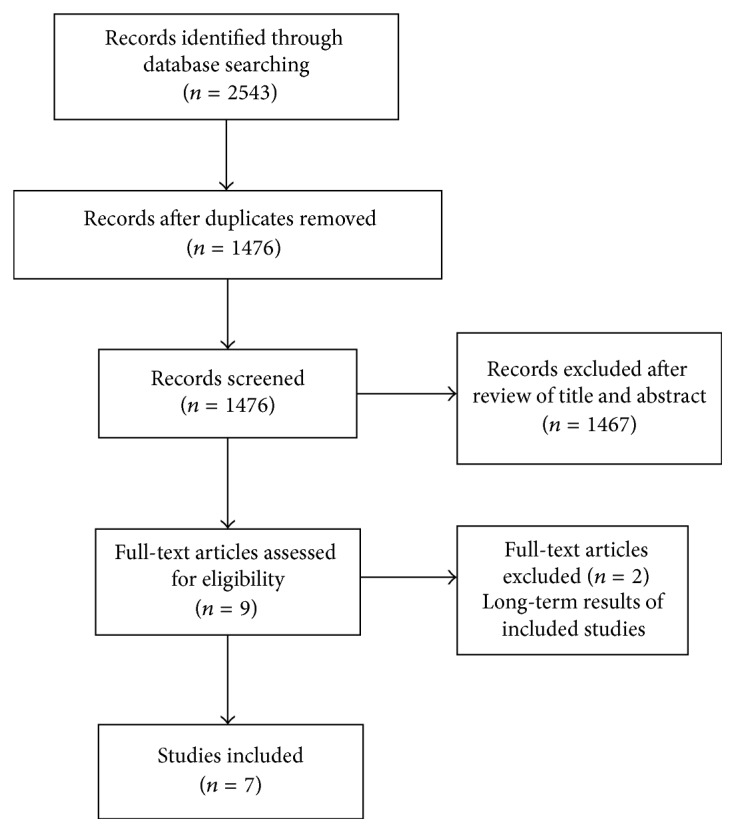
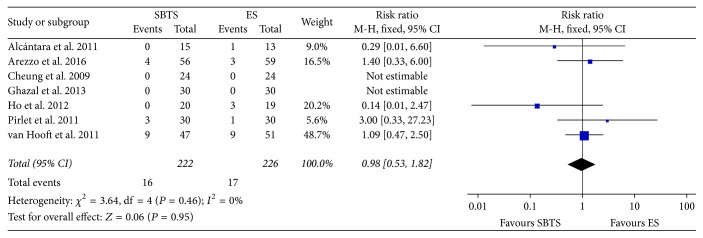
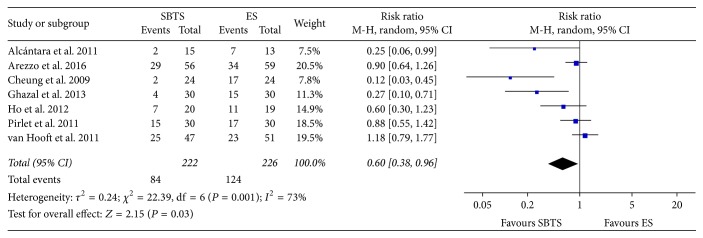
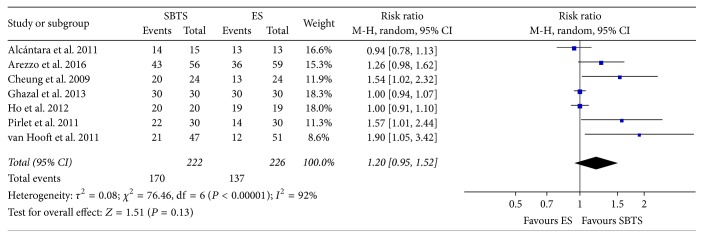
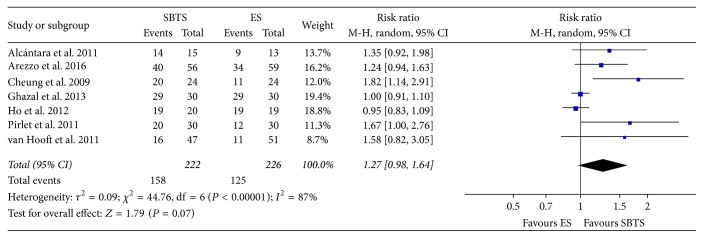
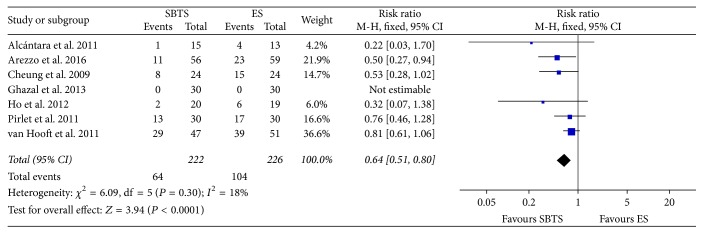
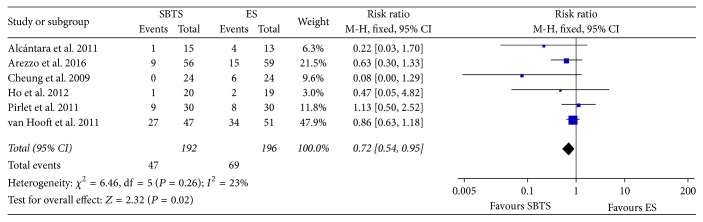
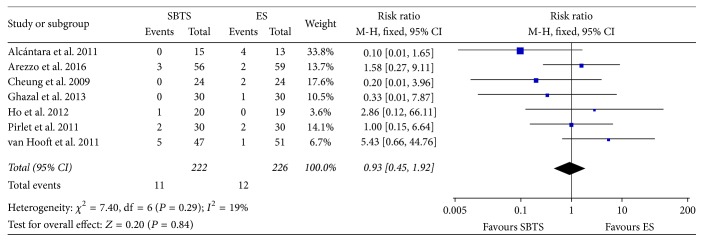
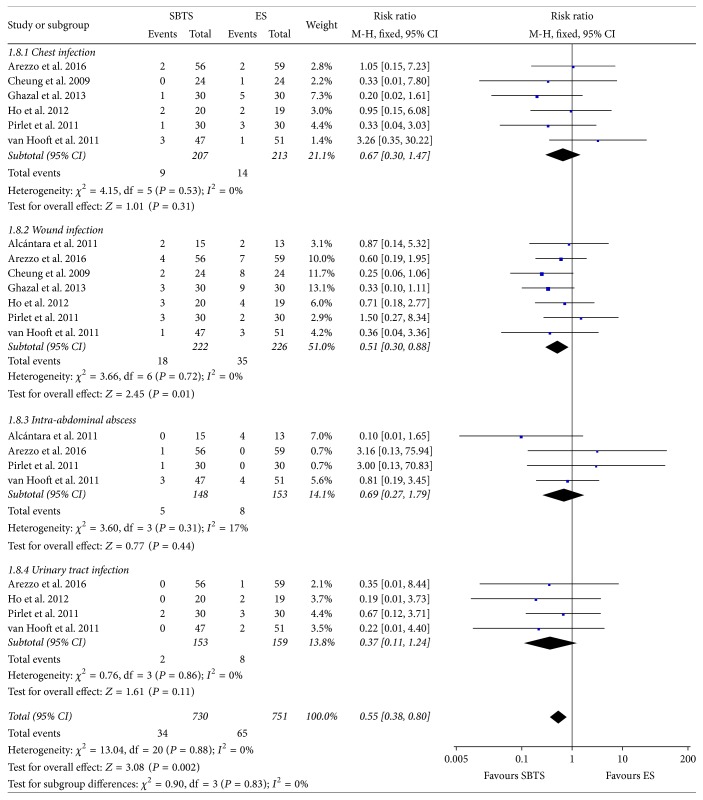
Results: We initially identified a total of 2543 studies. After the elimination of duplicates and the screening of titles and abstracts, seven studies, for a total of 448 patients, were considered. The current meta-analysis revealed no difference in the mortality rate between the stent group and the emergency surgery group; the postoperative complication rate (37.84% versus 54.87%, P = 0.02), the stoma rate (28.8% versus 46.02%, P < 0.0001), and the incidence of wound infection (8.11% versus 15.49%, P = 0.01) were reduced after stent as a bridge to surgery.
Conclusion: Colonic stenting as a bridge to surgery appears to be a safe approach to malignant large bowel obstruction. Possible advantages of this treatment can be identified in a reduced incidence of postoperative complications and a lower stoma rate. Further RCTs considering long-term outcomes and cost-effectiveness analysis are needed.
Figures
References
-
- Dohmoto M. New method-endoscopic implantation of rectal stent in palliative treatment of malignant stenosis. Digestive Endoscopy. 1991;3:1507–1512.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
