

Risk Factors for Prolonged Length of Hospital Stay and Readmissions After Laparoscopic Sleeve Gastrectomy and Laparoscopic Roux-en-Y Gastric Bypass
- PMID: 28762024
- PMCID: PMC5778173
- DOI: 10.1007/s11695-017-2844-x
Risk Factors for Prolonged Length of Hospital Stay and Readmissions After Laparoscopic Sleeve Gastrectomy and Laparoscopic Roux-en-Y Gastric Bypass
Abstract
Background: Laparoscopic sleeve gastrectomy (LSG) and laparoscopic gastric bypass (LRYGB) are most commonly performed bariatric procedures. Laparoscopic approach and enhanced recovery after surgery (ERAS) protocols managed to decrease length of hospital and morbidity. However, there are patients in whom, despite adherence to the protocol, the length of stay (LOS) remains longer than targeted. This study aimed to assess potential risk factors for prolonged LOS and readmissions.
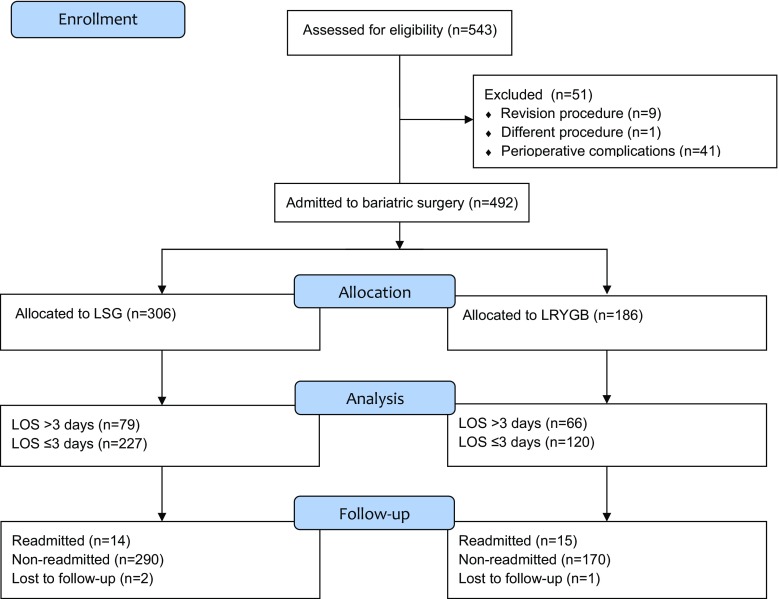
Methods: The study was a prospective observation with a post-hoc analysis of bariatric patients in a tertiary referral university teaching hospital. Inclusion criteria were undergoing laparoscopic bariatric surgery. Exclusion criteria were occurrence of perioperative complications, prior bariatric procedures, and lack of necessary data. The primary endpoints were the evaluations of risk factors for prolonged LOS and readmissions.
Results: Median LOS was 3 (2-4) days. LOS > 3 days occurred in 145 (29.47%) patients, 79 after LSG (25.82%) and 66 after LRYGB (35.48%; p = 0.008). Factors significantly prolonging LOS were low oral fluid intake, high intravenous volume of fluids administered on POD0, and every additional 50 km distance from habitual residence to bariatric center. The risk of hospital readmission rises with occurrence of intraoperative adverse events and low oral fluid intake on the day of surgery on.
Conclusions: Risk factors for prolonged LOS are low oral fluid intake, high intravenous volume of fluids administered on POD0, and every additional 50 km distance from habitual residence. Risk factors for hospital readmission are intraoperative adverse events and low oral fluid intake on the day of surgery.
Keywords: Bariatric surgery; Length of hospital stay; Readmission; Risk factors.
Conflict of interest statement
Conflict of Interest
The authors declare that they have no conflict of interest.
Consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Bioethics Committee of the Jagiellonian University.
Similar articles
-
Postoperative Care and Functional Recovery After Laparoscopic Sleeve Gastrectomy vs. Laparoscopic Roux-en-Y Gastric Bypass Among Patients Under ERAS Protocol.Obes Surg. 2018 Apr;28(4):1031-1039. doi: 10.1007/s11695-017-2964-3. Obes Surg. 2018. PMID: 29058236 Free PMC article.
-
Comparison of Early Morbidity and Mortality Between Sleeve Gastrectomy and Gastric Bypass in High-Risk Patients for Liver Disease: Analysis of American College of Surgeons National Surgical Quality Improvement Program.Obes Surg. 2018 Sep;28(9):2844-2851. doi: 10.1007/s11695-018-3259-z. Obes Surg. 2018. PMID: 29696572
-
Comparison of Outcomes Between Laparoscopic Roux-en-Y Gastric Bypass and Sleeve Gastrectomy in a Lebanese Bariatric Surgical Practice.Obes Surg. 2018 Feb;28(2):396-404. doi: 10.1007/s11695-017-2849-5. Obes Surg. 2018. PMID: 28776151
-
Does C-reactive Protein Have a Predictive Role in the Early Diagnosis of Postoperative Complications After Bariatric Surgery? Systematic Review and Bayesian Meta-analysis.Obes Surg. 2019 Nov;29(11):3448-3456. doi: 10.1007/s11695-019-04013-0. Obes Surg. 2019. PMID: 31240535
-
Learning Curves of Laparoscopic Roux-en-Y Gastric Bypass and Sleeve Gastrectomy in Bariatric Surgery: a Systematic Review and Introduction of a Standardization.Obes Surg. 2020 Feb;30(2):640-656. doi: 10.1007/s11695-019-04230-7. Obes Surg. 2020. PMID: 31664653
Cited by
-
Guidelines for Perioperative Care in Bariatric Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations: A 2021 Update.World J Surg. 2022 Apr;46(4):729-751. doi: 10.1007/s00268-021-06394-9. Epub 2022 Jan 4. World J Surg. 2022. PMID: 34984504 Free PMC article. Review.
-
Initial experience with laparoscopic revisional single anastomosis duodeno-ileal bypass (SADI-S) after failed sleeve gastrectomy.Wideochir Inne Tech Maloinwazyjne. 2023 Jun;18(2):298-304. doi: 10.5114/wiitm.2023.128683. Epub 2023 Jun 15. Wideochir Inne Tech Maloinwazyjne. 2023. PMID: 37680742 Free PMC article.
-
The length of hospital stay following bariatric surgery in Australia: the impact of patient, procedure, system and surgeon.ANZ J Surg. 2023 Dec;93(12):2833-2842. doi: 10.1111/ans.18575. Epub 2023 Jun 20. ANZ J Surg. 2023. PMID: 37338075 Free PMC article.
-
Is It Possible to Predict Weight Loss After Bariatric Surgery?-External Validation of Predictive Models.Obes Surg. 2021 Jul;31(7):2994-3004. doi: 10.1007/s11695-021-05341-w. Epub 2021 Mar 13. Obes Surg. 2021. PMID: 33712937 Free PMC article.
-
Safety and cost of performing laparoscopic sleeve gastrectomy with same day discharge at a large academic hospital.Surg Endosc. 2024 Apr;38(4):2212-2218. doi: 10.1007/s00464-024-10673-6. Epub 2024 Feb 20. Surg Endosc. 2024. PMID: 38379004
References
-
- Matłok M, et al. Reduction of the risk of rhabdomyolysis after bariatric surgery with lower fluid administration in the perioperative period: a cohort study. 2016. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
