

Hepatitis B cure: From discovery to regulatory approval
- PMID: 28762522
- PMCID: PMC6294322
- DOI: 10.1002/hep.29323
Hepatitis B cure: From discovery to regulatory approval
Abstract
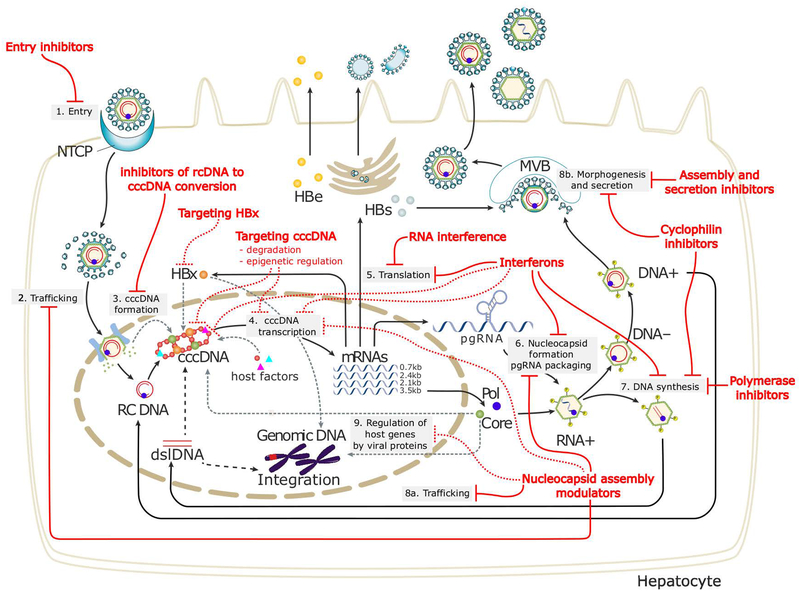
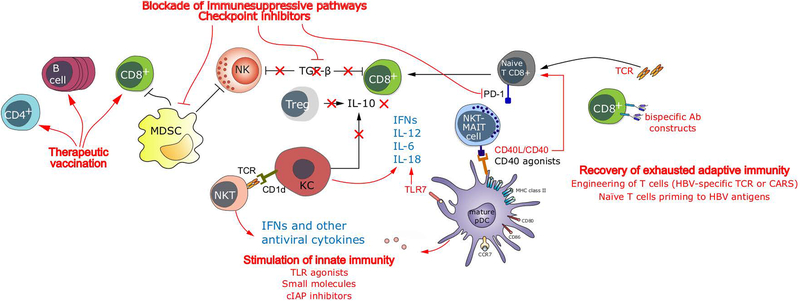
The majority of persons currently treated for chronic hepatitis B require long-term or lifelong therapy. New inhibitors of hepatitis B virus entry, replication, assembly, or secretion and immune modulatory therapies are in development. The introduction of these novel compounds for chronic hepatitis B necessitates a standardized appraisal of the efficacy and safety of these treatments and definitions of new or additional endpoints to inform clinical trials. To move the field forward and to expedite the pathway from discovery to regulatory approval, a workshop with key stakeholders was held in September 2016 to develop a consensus on treatment endpoints to guide the design of clinical trials aimed at hepatitis B cure. The consensus reached was that a complete sterilizing cure, i.e., viral eradication from the host, is unlikely to be feasible. Instead, a functional cure characterized by sustained loss of hepatitis B surface antigen with or without hepatitis B surface antibody seroconversion, which is associated with improved clinical outcomes, in a higher proportion of patients than is currently achieved with existing treatments is a feasible goal. Development of standardized assays for novel biomarkers toward better defining hepatitis B virus cure should occur in parallel with development of novel antiviral and immune modulatory therapies such that approval of new treatments can be linked to the approval of new diagnostic assays used to measure efficacy or to predict response. Combination of antiviral and immune modulatory therapies will likely be needed to achieve functional hepatitis B virus cure. Limited proof-of-concept monotherapy studies to evaluate safety and antiviral activity should be conducted prior to proceeding to combination therapies. The safety of any new curative therapies will be paramount given the excellent safety of currently approved nucleos(t)ide analogues. (Hepatology 2017).
© 2017 by the American Association for the Study of Liver Diseases, published by Wiley Periodicals, Inc., and © 2017 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
ASL has received research grant funding from Bristol-Myers Squibb and Gilead
FZ has received research grants and consulting fees from Arbutus, Assembly, Gilead, Janssen, Roche, Sanofi
GD has received research grants and consulting fees from Gilead Sciences, Janssen, Merck, AbbVie and Bristol Myers Squibb and has participated in safety monitoring boards for Regulus, Shionogi and Transgene.
MGG has no conflict to declare
Figures
Comment in
-
Checkpoint modulation in chronic hepatitis B: From hypothesis to approval.Hepatology. 2018 Mar;67(3):1175-1176. doi: 10.1002/hep.29695. Epub 2018 Jan 30. Hepatology. 2018. PMID: 29194685 No abstract available.
References
-
- Liaw YF, Sung JJ, Chow WC, et al. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med 2004;351:1521–31. - PubMed
-
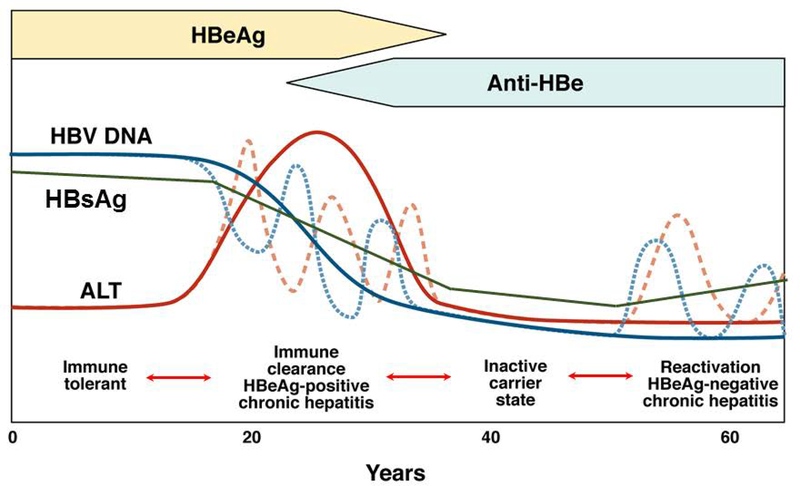
- Kennedy PT, Sandalova E, Jo J, et al. Preserved T-cell function in children and young adults with immune-tolerant chronic hepatitis B. Gastroenterology 2012;143:637–45. - PubMed
-
- Wu JF, Chiu YC, Chang KC, et al. Predictors of hepatitis B e antigen-negative hepatitis in chronic hepatitis B virus-infected patients from childhood to adulthood. Hepatology (Baltimore, Md) 2016;63:74–82. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
