

A comparison of operative outcomes between standard and robotic laparoscopic surgery for endometrial cancer: A systematic review and meta-analysis
- PMID: 28762635
- PMCID: PMC5724687
- DOI: 10.1002/rcs.1851
A comparison of operative outcomes between standard and robotic laparoscopic surgery for endometrial cancer: A systematic review and meta-analysis
Abstract
Background: Evidence has been systematically assessed comparing robotic with standard laparoscopy for treatment of endometrial cancer.
Methods: A search of Medline, Embase and Cochrane databases was performed until 30th October 2016.
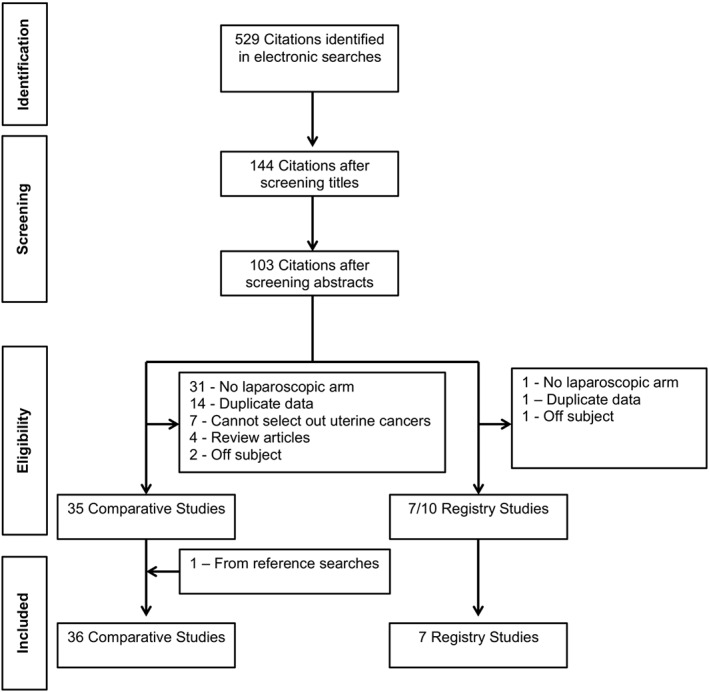
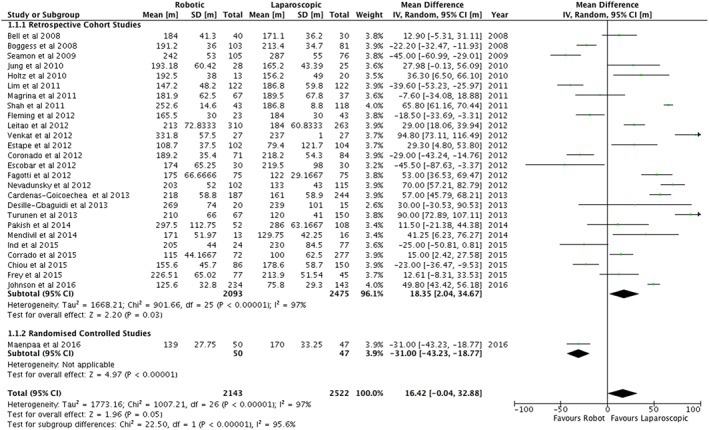
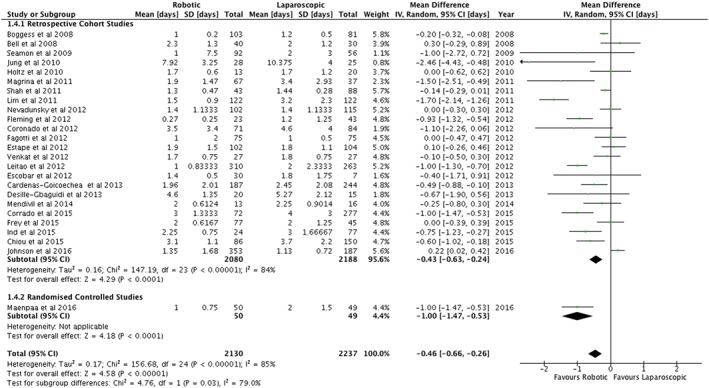
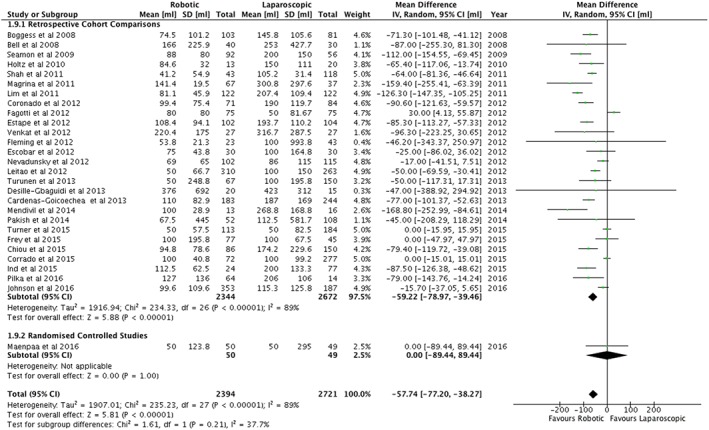
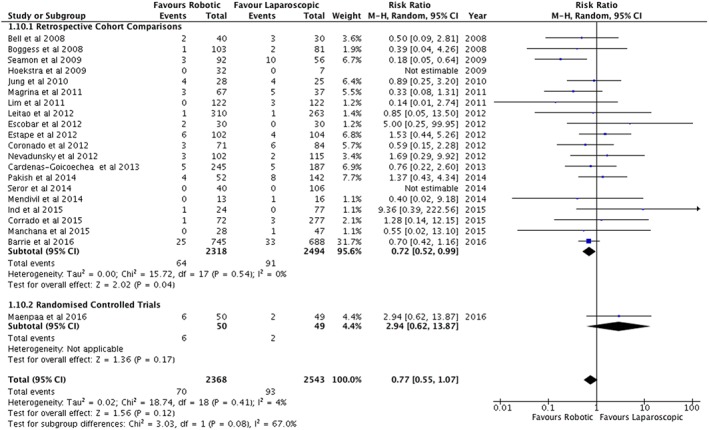
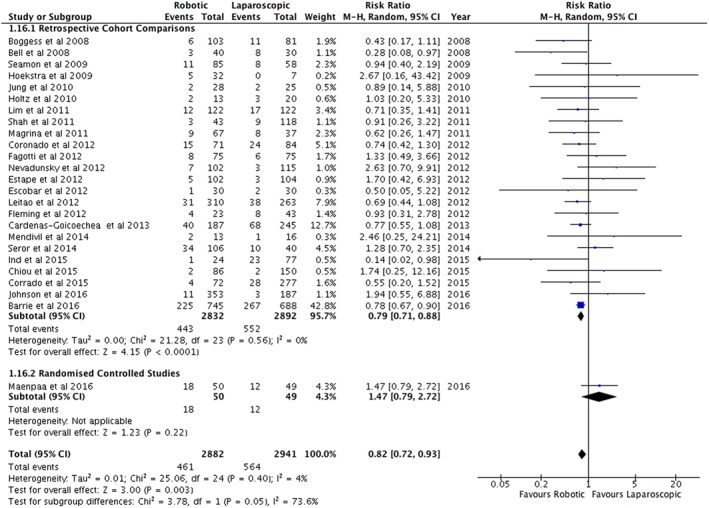
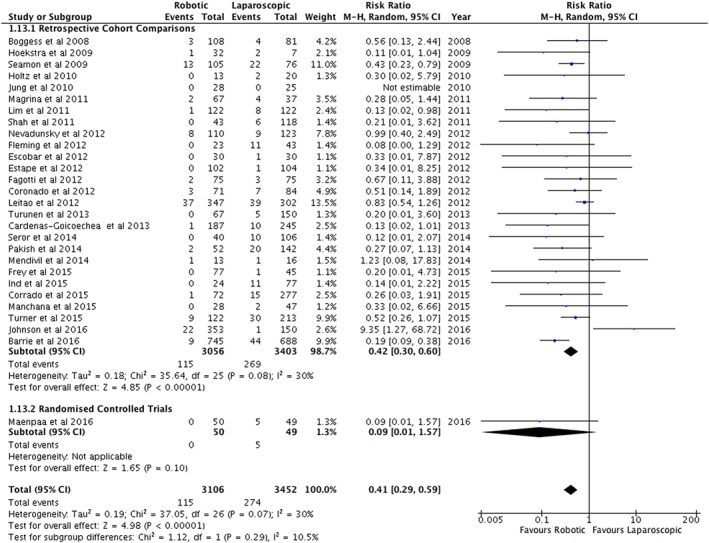
Results: Thirty-six papers including 33 retrospective studies, two matched case-control studies and one randomized controlled study were used in a meta-analysis. Information from a further seven registry/database studies were assessed descriptively. There were no differences in the duration of surgery but days stay in hospital were shorter in the robotic arm (0.46 days, 95%CI 0.26 to 0.66). A robotic approach had less blood loss (57.74 mL, 95%CI 38.29 to 77.20), less conversions to laparotomy (RR = 0.41, 95%CI 0.29 to 0.59), and less overall complications (RR = 0.82, 95%CI 0.72 to 0.93). A robotic approach had higher costs ($1746.20, 95%CI $63.37 to $3429.03).
Conclusion: A robotic approach has favourable clinical outcomes but is more expensive.
© 2017 The Authors. The International Journal of Medical Robotics and Computer Assisted Surgery Published by John Wiley & Sons Ltd.
Figures
References
-
- Galaal K, Bryant A, Fisher AD, Al‐Khaduri M, Kew F, Lopes AD. Laparoscopy versus laparotomy for the management of early stage endometrial cancer. Cochrane Database of Systematic Reviews. 2012;(9): https://doi.org/10.1002/14651858.CD006655.pub2 (published Online First: Epub Date) - DOI - PubMed
-
- Willis SF, Barton D, Ind TE. Laparoscopic hysterectomy with or without pelvic lymphadenectomy or sampling in a high‐risk series of patients with endometrial cancer. Int Seminars Surg Oncol: ISSO. 2006;3:28 https://doi.org/10.1186/1477–7800–3‐28 (published Online First: Epub Date) - DOI - PMC - PubMed
-
- Rashid TG, Kini M, Ind TE. Comparing the learning curve for robotically assisted and straight stick laparoscopic procedures in surgical novices. Int J Med Robot + Comput Assist Surg: MRCAS. 2010;6(3):306‐310. https://doi.org/10.1002/rcs.333 (published Online First: Epub Date) - DOI - PubMed
-
- Haider JN, Ind TE. Comparison of knot tying in robotic, laparoscopic, and open surgery: Robotic knots as tight as but more secure than open knots. J Gynecol Surg. 2013;29(6):287‐291.
-
- Ind TE, Marshall C, Hacking M, et al. Introducing robotic surgery into an endometrial cancer service ‐‐ a prospective evaluation of clinical and economic outcomes in a UK institution. Int J Med Robot + Comput Assist Surg: MRCAS. 2016;12(1):137‐144. https://doi.org/10.1002/rcs.1651 (published Online First: Epub Date) - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
