

Obesity and adverse breast cancer risk and outcome: Mechanistic insights and strategies for intervention
- PMID: 28763097
- PMCID: PMC5591063
- DOI: 10.3322/caac.21405
Obesity and adverse breast cancer risk and outcome: Mechanistic insights and strategies for intervention
Abstract
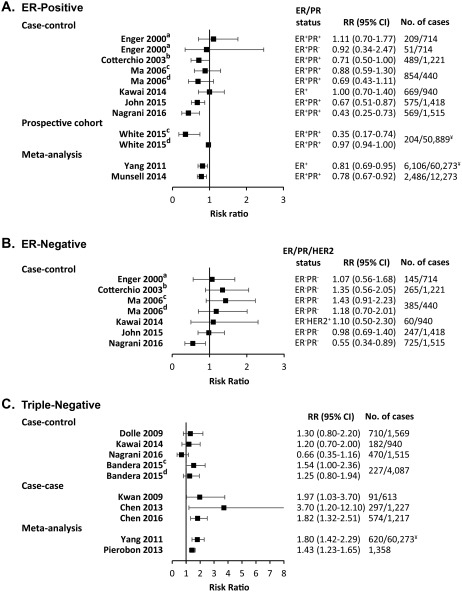
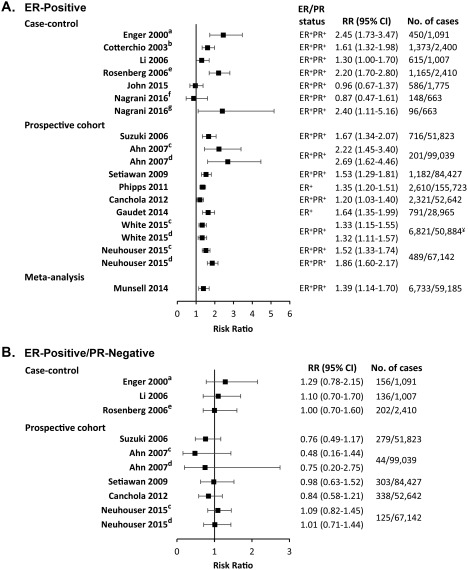
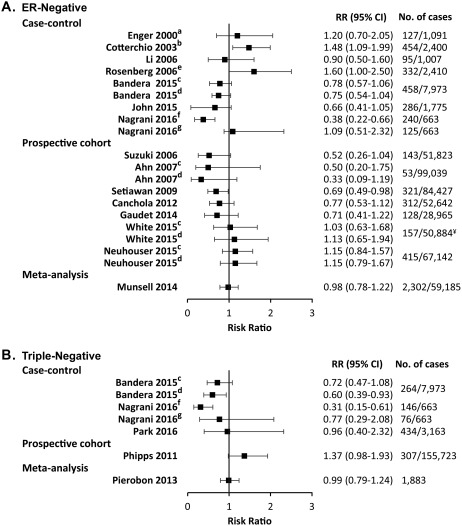
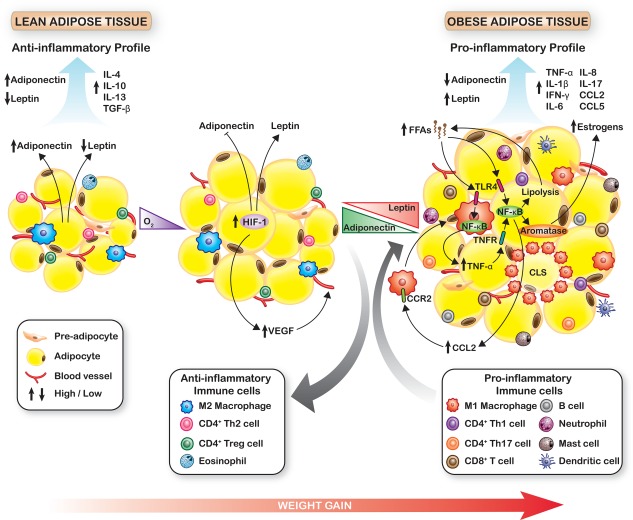
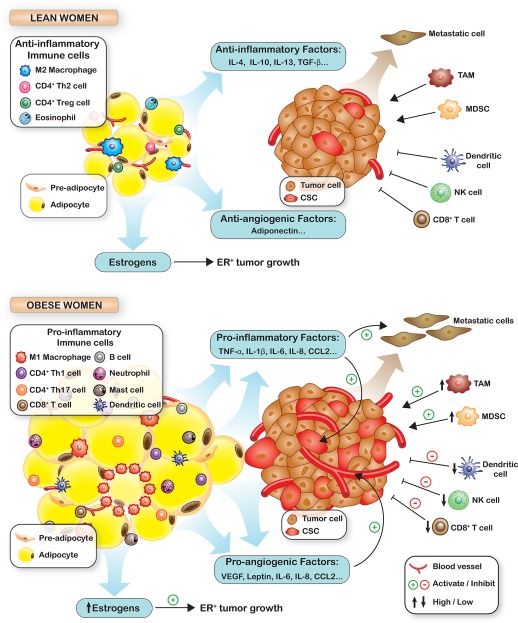
Answer questions and earn CME/CNE Recent decades have seen an unprecedented rise in obesity, and the health impact thereof is increasingly evident. In 2014, worldwide, more than 1.9 billion adults were overweight (body mass index [BMI], 25-29.9 kg/m2 ), and of these, over 600 million were obese (BMI ≥30 kg/m2 ). Although the association between obesity and the risk of diabetes and coronary artery disease is widely known, the impact of obesity on cancer incidence, morbidity, and mortality is not fully appreciated. Obesity is associated both with a higher risk of developing breast cancer, particularly in postmenopausal women, and with worse disease outcome for women of all ages. The first part of this review summarizes the relationships between obesity and breast cancer development and outcomes in premenopausal and postmenopausal women and in those with hormone receptor-positive and -negative disease. The second part of this review addresses hypothesized molecular mechanistic insights that may underlie the effects of obesity to increase local and circulating proinflammatory cytokines, promote tumor angiogenesis and stimulate the most malignant cancer stem cell population to drive cancer growth, invasion, and metastasis. Finally, a review of observational studies demonstrates that increased physical activity is associated with lower breast cancer risk and better outcomes. The effects of recent lifestyle interventions to decrease sex steroids, insulin/insulin-like growth factor-1 pathway activation, and inflammatory biomarkers associated with worse breast cancer outcomes in obesity also are discussed. Although many observational studies indicate that exercise with weight loss is associated with improved breast cancer outcome, further prospective studies are needed to determine whether weight reduction will lead to improved patient outcomes. It is hoped that several ongoing lifestyle intervention trials, which are reviewed herein, will support the systematic incorporation of weight loss intervention strategies into care for patients with breast cancer. CA Cancer J Clin 2017;67:378-397. © 2017 American Cancer Society.
Keywords: breast cancer; diet and exercise; hormone receptor; immunity; inflammatory cytokines; nuclear factor kappa B (NF-κB); obesity; postmenopausal and premenopausal; sex steroids; weight loss.
© 2017 The Authors. CA A Cancer Journal for Clinicians published by Wiley Periodicals, Inc. on behalf of American Cancer Society.
Figures
References
-
- World Health Organization . Obesity and Overweight. Fact Sheet 311 (Reviewed May 2014). Geneva, Switzerland: World Health Organization; 2014.
-
- Ogden CL, Carroll MD, Fryar CD, Flegal KM. Prevalence of Obesity Among Adults and Youth: United States, 2011‐2014. NCHS Data Brief, no. 201. Hyattsville, MD: National Center for Health Statistics; 2015. - PubMed
-
- International Agency for Research on Cancer/World Health Organization . Weight Control and Physical Activity. IARC Handbook of Cancer Prevention. Vol 6 Lyon, France: IARC Publications; 2002.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
