

Femur first surgical technique: a smart non-computer-based procedure to achieve the combined anteversion in primary total hip arthroplasty
- PMID: 28764697
- PMCID: PMC5539744
- DOI: 10.1186/s12891-017-1688-9
Femur first surgical technique: a smart non-computer-based procedure to achieve the combined anteversion in primary total hip arthroplasty
Abstract
Background: The relevance of prosthetic component orientation to prevent dislocation and impingement following total hip arthroplasty (THA) has been widely accepted. We investigated the use of a non-computer-based surgery to address the reciprocal orientation of the acetabular and femoral components.
Methods: In the femur first technique, the cup is positioned relative to the stem. When the definitive antetorsion of femoral component is fixed, the cup is positioned in a compliant anteversion to the stem. Clinical and radiographic assessments were performed before and 3 months after THA. Radiographic assessment was performed in standing position with the EOS 2D/3D radiography system. 3D images were used to preoperative anterior pelvic plane (APP) angle, postoperative acetabular inclination (AI) and anteversion (AA), and postoperative stem antetorsion. Clinical assessment was performed with Harris Hip Score (HHS).
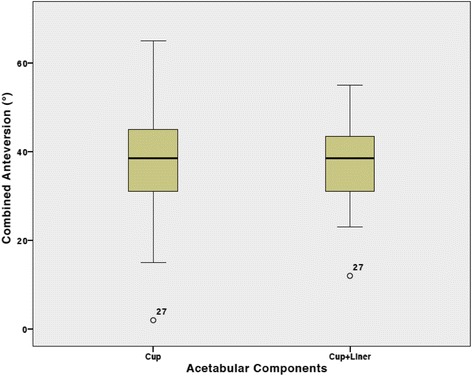
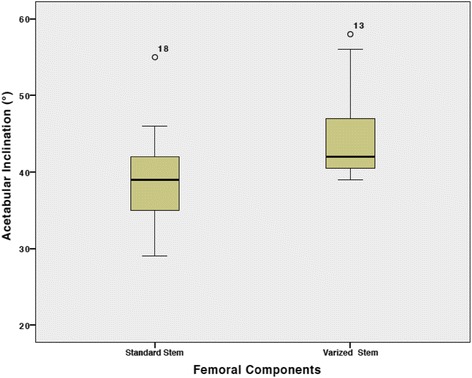
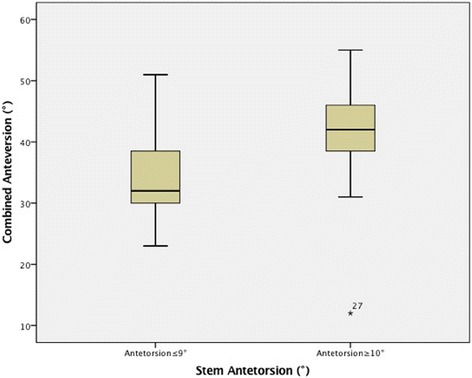
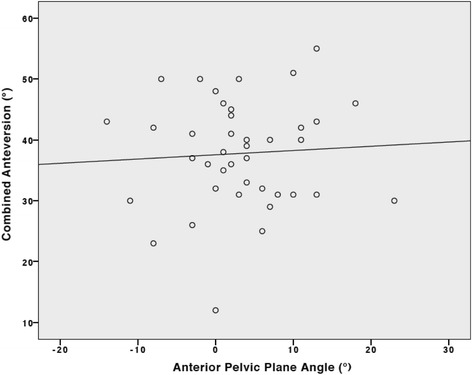
Results: Forty patients (40 hips) underwent primary THA with an average age of 61 years (range, 36-84). Average HHS increased from 43 ± 5 (range, 37-52) preoperatively to 97 ± 6 (range, 86-100) at the last follow-up (P < 0.0001). Average combined anteversion value of cup with liner and stem was 38° ± 9° (range, 12°-55°). Average AI value of cup with liner was 39° ± 6° (range, 30°-55°) in the group with standard stem and 45° ± 7° (range, 39°-58°) in the group with varized stem (P = 0.007). Relationship analysis showed no correlation between the combined anteversion values of the cup with liner and stem with APP angle values (r = 0.26, P = 0.87).
Conclusions: Femur first technique allows the surgeon to achieve a combined anteversion ranging from 25° to 50° with a cup inclination ranging from 30° to 50°. The cup is positioned according to the functional plane of the patient regardless the preoperative pelvic tilt.
Keywords: Acetabular inclination; Arthroplasty; Combined anteversion; Femur first; Hip.
Conflict of interest statement
Ethics approval and consent to participate
The present study was approved by the Independent Ethics Committee of Humanitas Clinical and Research Centre (protocol n.1366). All enrolled patients gave their consent to participate in the study.
Consent for publication
Not applicable.
Competing interests
One author (GG) is a paid consultant for Zimmer Biomet. Two authors (ML and UGL) are members of the Editorial Board of BMC Musculoskeletal Disorders. None of the other authors have any competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Del Schutte H, Jr., Lipman AJ, Bannar SM, Livermore JT, Ilstrup D, Morrey BF. Effects of acetabular abduction on cup wear rates in total hip arthroplasty. J Arthroplast 1998;13(6):621-626. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
