

Heart Failure Increases the Risk of Adverse Renal Outcomes in Patients With Normal Kidney Function
- PMID: 28765150
- PMCID: PMC5557387
- DOI: 10.1161/CIRCHEARTFAILURE.116.003825
Heart Failure Increases the Risk of Adverse Renal Outcomes in Patients With Normal Kidney Function
Abstract
Background: Heart failure (HF) is associated with poor cardiac outcomes and mortality. It is not known whether HF leads to poor renal outcomes in patients with normal kidney function. We hypothesized that HF is associated with worse long-term renal outcomes.
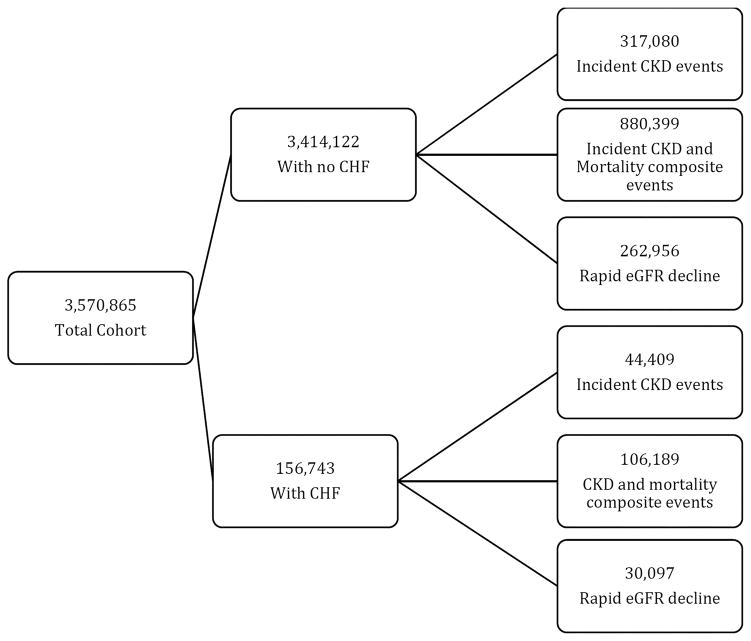
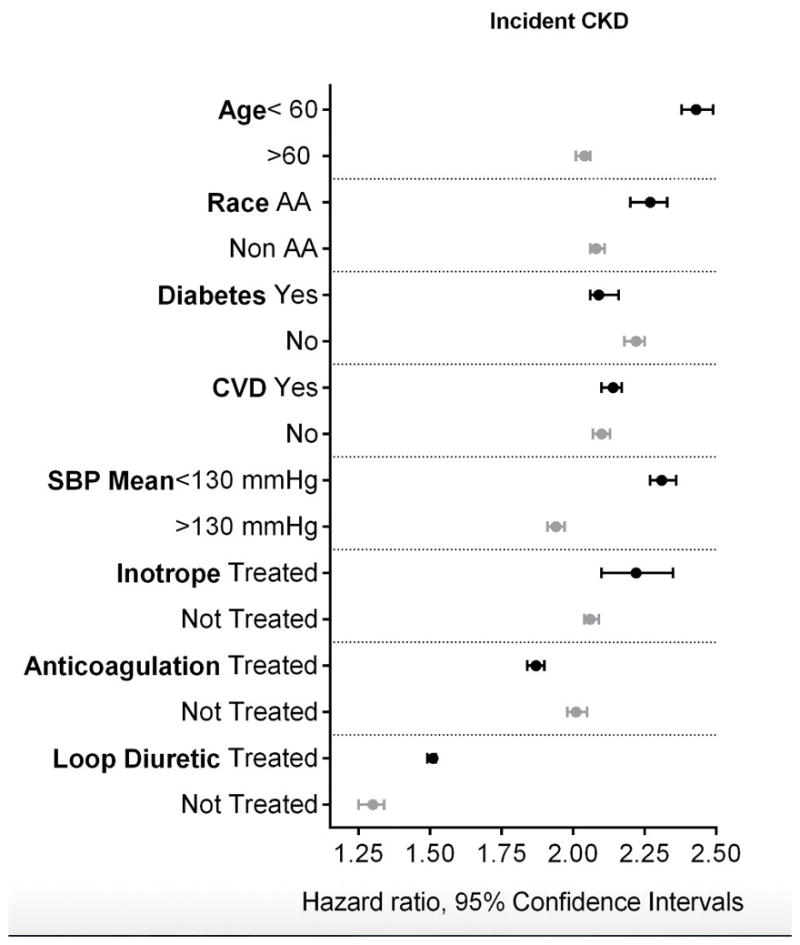
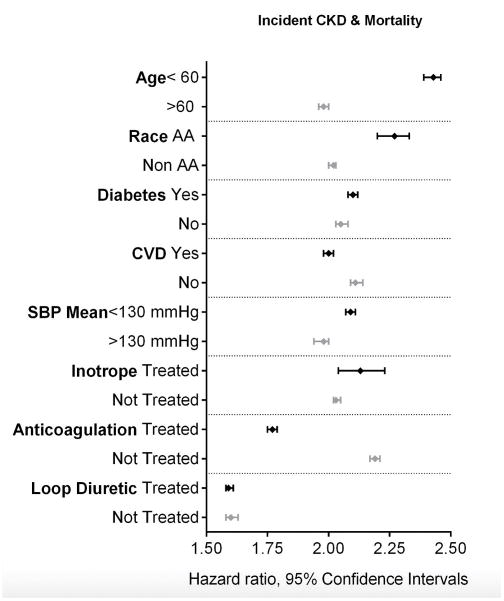
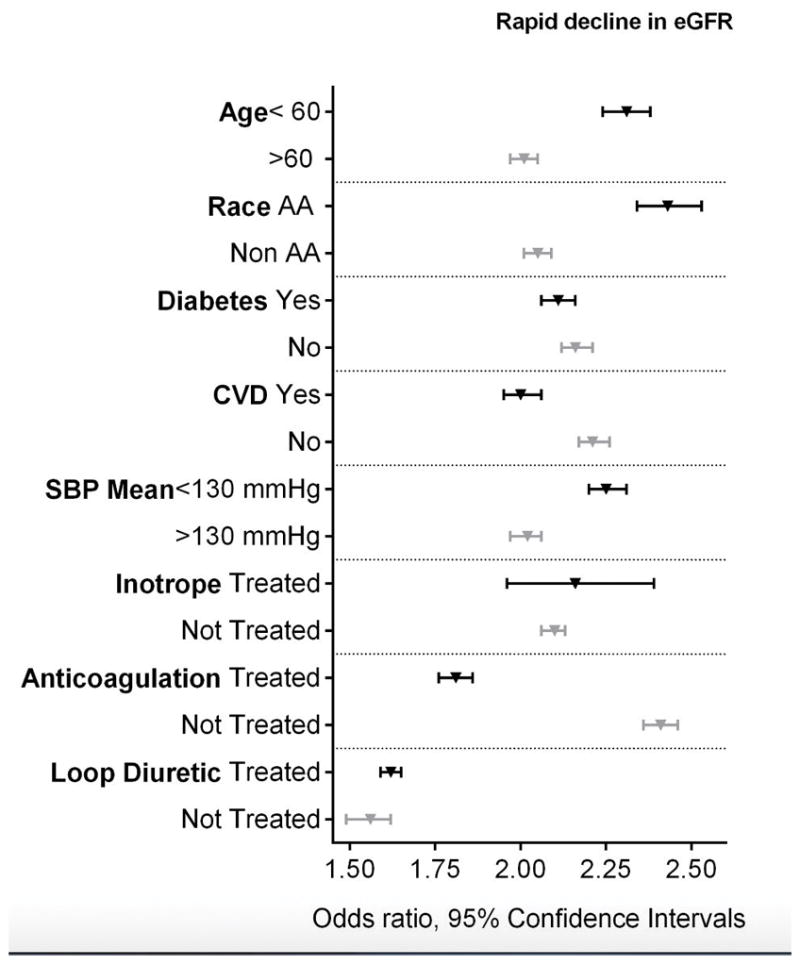
Methods and results: Among 3 570 865 US veterans with estimated glomerular filtration rate (eGFR) ≥60 mL min-1 1.73 m-2 during October 1, 2004 to September 30, 2006, we identified 156 743 with an International Classification of Diseases, Ninth Revision, diagnosis of HF. We examined the association of HF with incident chronic kidney disease (CKD), the composite of incident CKD or mortality, and rapid rate of eGFR decline (slopes steeper than -5 mL min-1 1.73 m-2 y-1) using Cox proportional hazard analyses and logistic regression. Adjustments were made for various confounders. The mean±standard deviation baseline age and eGFR of HF patients were 68±11 years and 78±14 mL min-1 1.73 m-2 and in patients without HF were 59±14 years and 84±16 mL min-1 1.73 m-2, respectively. HF patients had higher prevalence of hypertension, diabetes mellitus, cardiac, peripheral vascular and chronic lung diseases, stroke, and dementia. Incidence of CKD was 69.0/1000 patient-years in HF patients versus 14.5/1000 patient-years in patients without HF, and 22% of patients with HF had rapid decline in eGFR compared with 8.5% in patients without HF. HF patients had a 2.12-, 2.06-, and 2.13-fold higher multivariable-adjusted risk of incident CKD, composite of CKD or mortality, and rapid eGFR decline, respectively.
Conclusions: HF is associated with significantly higher risk of incident CKD, incident CKD or mortality, and rapid eGFR decline. Early diagnosis and management of HF could help reduce the risk of long-term renal complications.
Keywords: glomerular filtration rate; heart failure; incidence; kidney diseases; mortality; renal insufficiency; veterans.
© 2017 American Heart Association, Inc.
Conflict of interest statement
Figures
References
-
- Leithe ME, Margorien RD, Hermiller JB, Unverferth DV, Leier CV. Relationship between central hemodynamics and regional blood flow in normal subjects and in patients with congestive heart failure. Circulation. 1984;69:57–64. - PubMed
-
- Ljungman S, Laragh JH, Cody RJ. Role of the kidney in congestive heart failure. Relationship of cardiac index to kidney function. Drugs. 1990;39(Suppl 4):10–21. discussion 22–4. - PubMed
-
- McClellan WM, Langston RD, Presley R. Medicare patients with cardiovascular disease have a high prevalence of chronic kidney disease and a high rate of progression to end-stage renal disease. J Am Soc Nephrol. 2004;15:1912–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
