

Lauren subtypes of advanced gastric cancer influence survival and response to chemotherapy: real-world data from the AGAMENON National Cancer Registry
- PMID: 28765618
- PMCID: PMC5589993
- DOI: 10.1038/bjc.2017.245
Lauren subtypes of advanced gastric cancer influence survival and response to chemotherapy: real-world data from the AGAMENON National Cancer Registry
Abstract
Background: The choice of chemotherapy in HER2-negative gastric cancer is based on centre's preferences and adverse effects profile. No schedule is currently accepted as standard, nor are there any factors to predict response, other than HER2 status. We seek to evaluate whether Lauren type influences the efficacy of various chemotherapies and on patient overall survival (OS).
Methods: We have conducted a multicenter study in 31 hospitals. The eligibility criteria include diagnosis of stomach or gastroesophageal junction adenocarcinoma, HER2 negativity, and chemotherapy containing 2-3 drugs. Cox proportional hazards regression adjusted for confounding factors, with tests of 'treatment-by-histology' interaction, was used to estimate treatment effect.
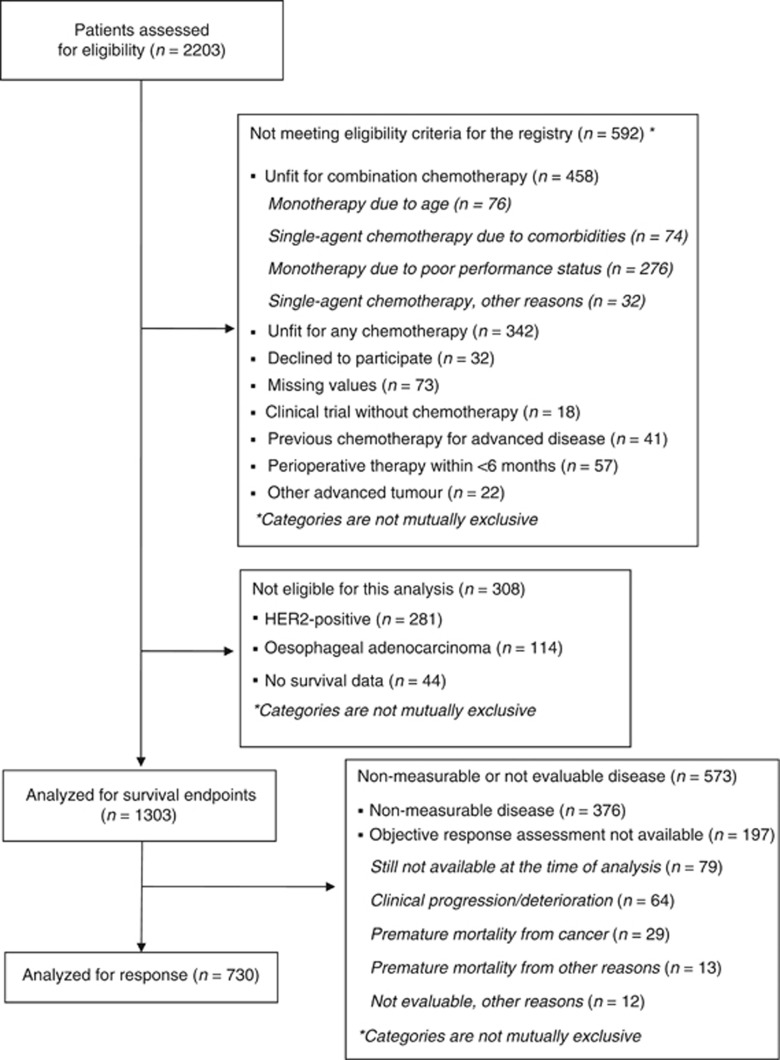
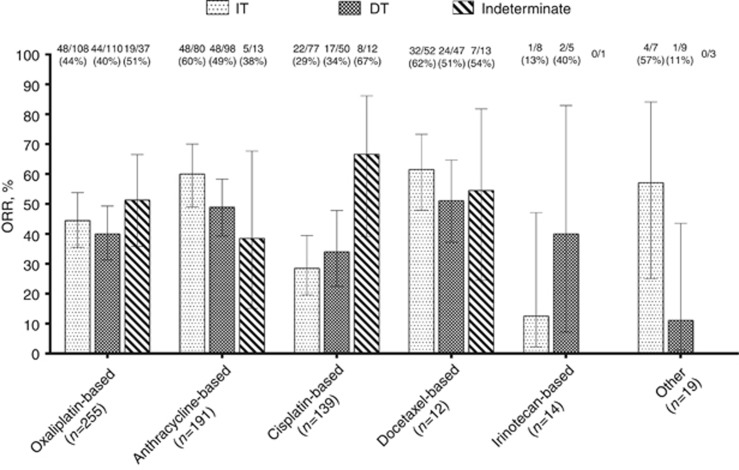
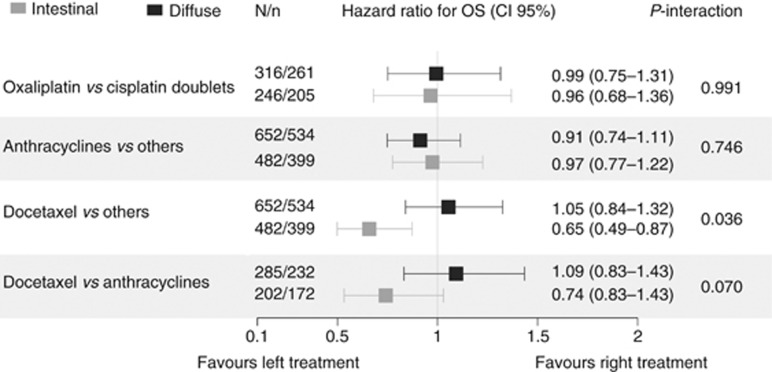
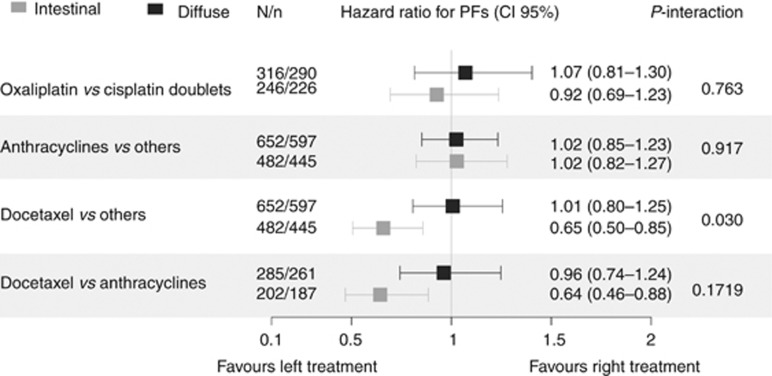
Results: Our registry contains 1303 tumours analysable for OS end points and 730 evaluable for overall response rate (ORR). A decrease in ORR was detected in the presence of a diffuse component: odds ratio 0.719 (95% confidence interval (CI), 0.525-0.987), P=0.039. Anthracycline- or docetaxel-containing schedules increased ORR only in the intestinal type. The diffuse type displayed increased mortality with hazard ratio (HR) of 1.201 (95% CI, 1.054-1.368), P=0.0056. Patients receiving chemotherapy with docetaxel exhibited increased OS limited to the intestinal type: HR 0.65 (95% CI, 0.49-0.87), P=0.024, with no increment in OS for the subset having a diffuse component. With respect to progression-free survival (PFS), a significant interaction was seen in the effect of docetaxel-containing schedules, with better PFS limited to the intestinal type subgroup, in the comparison against any other schedule: HR 0.65 (95% CI, 0.50-0.85), P=0.015, and against anthracycline-based regimens: HR 0.64 (95% CI, 0.46-0.88), P=0.046.
Conclusions: As a conclusion, in this registry, Lauren classification tumour subtypes predicted survival and responded differently to chemotherapy. Future clinical trials should stratify effect estimations based on histology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ajani JA, Rodriquez W, Bodoky G, Moiseyenko V, Lichinitser M, Gorbunova V, Vynnychenko I, Garin A, Lang I, Falcon S (2009) Multicenter phase III comparison of cisplatin/S-1 (CS) with cisplatin/5-FU (CF) as first-line therapy in patients with advanced gastric cancer (FLAGS): Secondary and subset analyses. In: ASCO Annual Meeting Proceedings. J Clin Oncol27(suppl 15): 4511.
-
- Al-Batran S-E, Hofheinz RD, Pauligk C, Kopp H-G, Haag GM, Luley KB, Meiler J, Homann N, Lorenzen S, Schmalenberg H, Probst S, Koenigsmann M, Egger M, Prasnikar N, Caca K, Trojan J, Martens UM, Block A, Fischbach W, Mahlberg R, Clemens M, Illerhaus G, Zirlik K, Behringer DM, Schmiegel W, Pohl M, Heike M, Ronellenfitsch, Schuler M, Bechstein WO, Königsrainer A, Gaiser T, Schirmacher P, Hozaeel W, Reichart A, Goetze TO, Sievert M, Jäger E, Mönig S, Tannapfel A (2016) Histopathological regression after neoadjuvant docetaxel, oxaliplatin, fluorouracil, and leucovorin versus epirubicin, cisplatin, and fluorouracil or capecitabine in patients with resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4-AIO). Lancet Oncol 17: 1697–1708. - PubMed
-
- Bang YJ, Van Cutsem E, Feyereislova A, Chung HC, Shen L, Sawaki A, Lordick F, Ohtsu A, Omuro Y, Satoh T, Aprile G, Kulikov E, Hill J, Lehle M, Rüschoff J, Kang YK (2010) Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 376: 687–697. - PubMed
-
- Barraclough H, Govindan R (2010) Biostatistics primer: what a clinician ought to know: subgroup analyses. J Thorac Oncol 5: 741–746. - PubMed
-
- Boku N, Yamamoto S, Fukuda H, Shirao K, Doi T, Sawaki A, Koizumi W, Saito H, Yamaguchi K, Takiuchi H, Nasu J, Ohtsu A (2009) Fluorouracil versus combination of irinotecan plus cisplatin versus S-1 in metastatic gastric cancer: a randomised phase 3 study. Lancet Oncol 10: 1063–1069. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
