

Effect of initial stent position on patency of transjugular intrahepatic portosystemic shunt
- PMID: 28765699
- PMCID: PMC5514643
- DOI: 10.3748/wjg.v23.i26.4779
Effect of initial stent position on patency of transjugular intrahepatic portosystemic shunt
Abstract
Aim: To evaluate the effect of initial stent position on transjugular intrahepatic portosystemic shunt (TIPS).
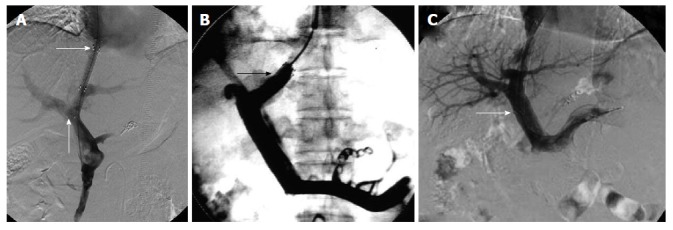
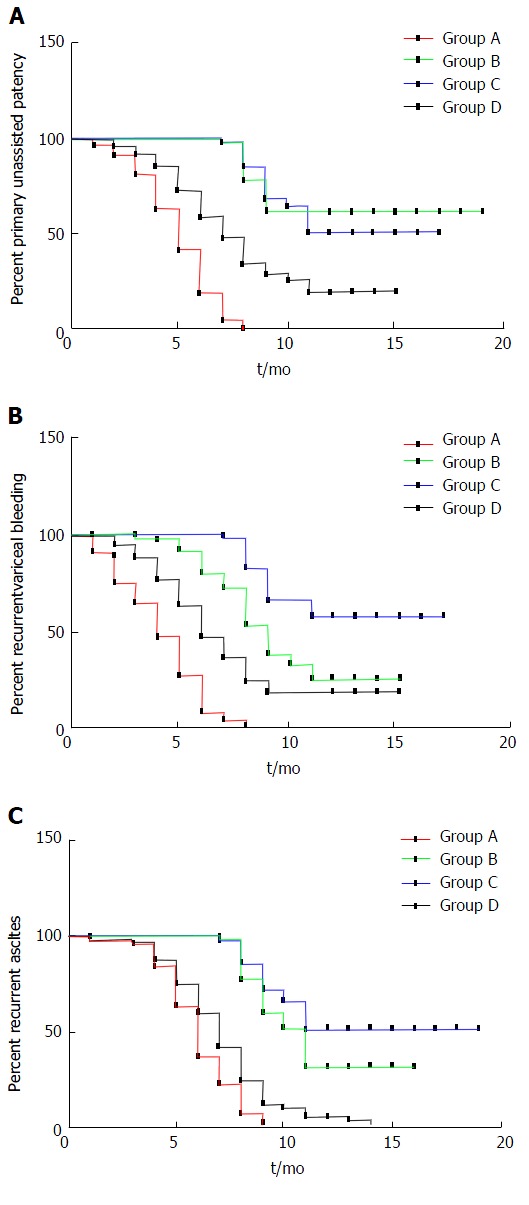
Methods: We studied 425 patients from January 2004 to January 2015 with refractory ascites or variceal bleeding who required TIPS placement. Patients were randomly divided into group A (stent in hepatic vein, n = 57), group B (stent extended to junction of hepatic vein and inferior vena cava, n = 136), group C (stent in left branch of portal vein, n = 83) and group D (stent in main portal vein, n = 149). Primary unassisted patency was compared using Kaplan-Meier analysis, and incidence of recurrence of bleeding, ascites and hepatic encephalopathy (HE) were analyzed.
Results: The mean primary unassisted patency rate in group B tended to be higher than in group A at 3, 6 and 12 mo (P = 0.001, 0.000 and 0.005), and in group D it tended to be lower than in group C at 3, 6 and 12 mo (P = 0.012, 0.000 and 0.028). The median shunt primary patency time for group A was shorter than for group B (5.2 mo vs 9.1 mo, 95%CI: 4.3-5.6, P = 0.013, log-rank test), while for group C it was longer than for group D (8.3 mo vs 6.9 mo, 95%CI: 6.3-7.6, P = 0.025, log-rank test). Recurrence of bleeding and ascites in group A was higher than in group B at 3 mo (P = 0.014 and 0.020), 6 mo (P = 0.014 and 0.019) and 12 mo (P = 0.024 and 0.034. Recurrence in group D was higher than in group C at 3 mo (P = 0.035 and 0.035), 6 mo (P = 0.038 and 0.022) and 12 mo (P = 0.017 and 0.009). The incidence of HE was not significantly different among any of the groups (P = 0.965).
Conclusion: The initial stent position can markedly affect stent patency, which potentially influences the risk of recurrent symptoms associated with shunt stenosis or occlusion.
Keywords: Liver cirrhosis; Portal hypertension; Stent position; Transjugular intrahepatic portosystemic shunt.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that there is no conflict of interest related to this study.
Figures
References
-
- García-Pagán JC, Caca K, Bureau C, Laleman W, Appenrodt B, Luca A, Abraldes JG, Nevens F, Vinel JP, Mössner J, et al. Early use of TIPS in patients with cirrhosis and variceal bleeding. N Engl J Med. 2010;362:2370–2379. - PubMed
-
- Nardelli S, Gioia S, Pasquale C, Pentassuglio I, Farcomeni A, Merli M, Salvatori FM, Nikolli L, Torrisi S, Greco F, et al. Cognitive Impairment Predicts The Occurrence Of Hepatic Encephalopathy After Transjugular Intrahepatic Portosystemic Shunt. Am J Gastroenterol. 2016;111:523–528. - PubMed
-
- Rössle M. TIPS: 25 years later. J Hepatol. 2013;59:1081–1093. - PubMed
-
- Rösch J, Keller FS. Transjugular intrahepatic portosystemic shunt: present status, comparison with endoscopic therapy and shunt surgery, and future prospectives. World J Surg. 2001;25:337–345; discussion 345-346. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
