

Simulation of Lipid-Lowering Therapy Intensification in a Population With Atherosclerotic Cardiovascular Disease
- PMID: 28768335
- PMCID: PMC5710173
- DOI: 10.1001/jamacardio.2017.2289
Simulation of Lipid-Lowering Therapy Intensification in a Population With Atherosclerotic Cardiovascular Disease
Abstract
Importance: In patients with atherosclerotic cardiovascular disease (ASCVD), guidelines recommend optimizing statin treatment, and consensus pathways suggest use of ezetimibe and proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors in patients with persistently elevated low-density lipoprotein cholesterol (LDL-C) levels despite use of statins. Recent trials have provided evidence of benefit in reduction of cardiovascular events with these agents.
Objective: To estimate the percentage of patients with ASCVD who would require a PCSK9 inhibitor when oral lipid-lowering therapy (LLT) is intensified first.
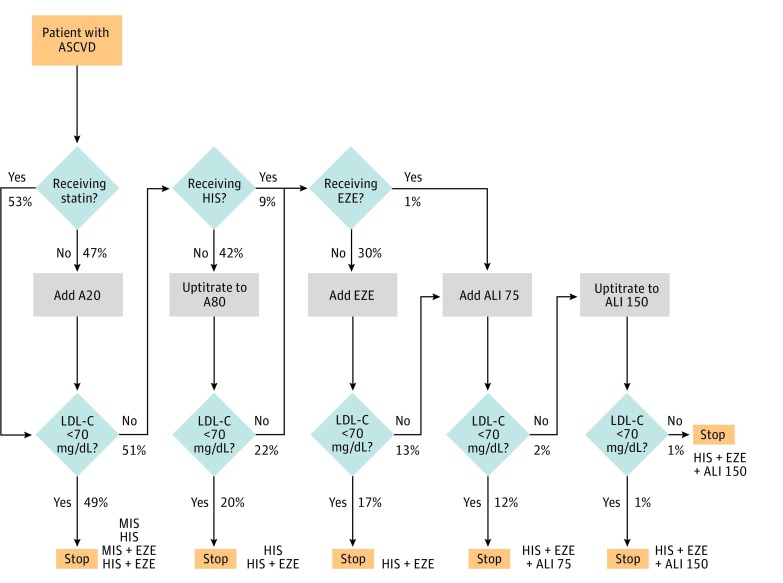
Design, setting, and participants: This simulation model study used a large administrative database of US medical and pharmacy claims to identify a cohort of 105 269 patients with ASCVD enrolled from January 1, 2012, through December 31, 2013, who met the inclusion criteria (database cohort). Patients were sampled with replacement (bootstrapping) to match the US epidemiologic distribution and entered into a Monte Carlo simulation (simulation cohort) that applied stepwise treatment intensification algorithms in those with LDL-C levels of at least 70 mg/dL. All patients not initially receiving a statin were given atorvastatin, 20 mg, and the following LLT intensification steps were applied: uptitration to atorvastatin, 80 mg; add-on ezetimibe therapy; add-on alirocumab therapy, 75 mg (a PCSK9 inhibitor); and uptitration to alirocumab, 150 mg. Sensitivity analyses included evolocumab as a PCSK9 inhibitor. Efficacy was estimated from published studies and incorporated patient-level variation. Data were analyzed from December 2015 to May 2017.
Exposures: Treatment intensification strategies with LLT.
Main outcomes and measures: Use of LLT among the population with ASCVD and distributions of LDL-C levels under various treatment intensification scenarios.
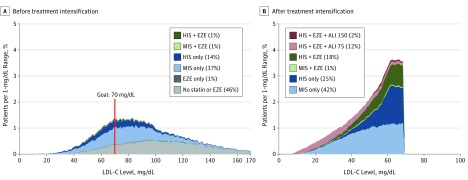
Results: Inclusion criteria were met by 105 269 individuals in the database cohort (57.2% male and 42.8% female; mean [SD] age, 65.1 [12.1] years). In the simulation cohort (1 million patients; 54.8% male and 45.2% female; mean [SD] age, 66.4 [12.2] years), before treatment intensification, 51.5% used statin monotherapy and 1.7% used statins plus ezetimibe. Only 25.2% achieved an LDL-C level of less than 70 mg/dL. After treatment intensification, 99.3% could achieve an LDL-C level of less than 70 mg/dL, including 67.3% with statin monotherapy, 18.7% with statins plus ezetimibe, and 14% with add-on PCSK9 inhibitor.
Conclusions and relevance: Large gaps exist between recommendations and current practice regarding LLT in the population with ASCVD. In our model that assumes no LLT intolerance and full adherence, intensification of oral LLT could achieve an LDL-C level of less than 70 mg/dL in most patients, with only a modest percentage requiring a PCSK9 inhibitor.
Conflict of interest statement
Figures
Comment in
-
Defining Potential Use of Nonstatin Therapies to Lower Blood Cholesterol Levels.JAMA Cardiol. 2017 Sep 1;2(9):946-947. doi: 10.1001/jamacardio.2017.2290. JAMA Cardiol. 2017. PMID: 28768332 No abstract available.
-
Simulation Models of Therapy Intensification in Lipid-Lowering Medicine-Reply.JAMA Cardiol. 2018 Jan 1;3(1):89. doi: 10.1001/jamacardio.2017.4353. JAMA Cardiol. 2018. PMID: 29188279 No abstract available.
-
Simulation Models of Therapy Intensification in Lipid-Lowering Medicine: Fact or Fantasy?JAMA Cardiol. 2018 Jan 1;3(1):88-89. doi: 10.1001/jamacardio.2017.4344. JAMA Cardiol. 2018. PMID: 29188280 No abstract available.
References
-
- Mihaylova B, Emberson J, Blackwell L, et al. ; Cholesterol Treatment Trialists’ (CTT) Collaborators . The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet. 2012;380(9841):581-590. - PMC - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH, et al. ; American College of Cardiology/American Heart Association Task Force on Practice Guidelines . 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25, pt B):2889-2934. - PubMed
-
- Cannon CP, Blazing MA, Giugliano RP, et al. ; IMPROVE-IT Investigators . Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372(25):2387-2397. - PubMed
-
- Murphy SA, Cannon CP, Blazing MA, et al. . Reduction in total cardiovascular events with ezetimibe/simvastatin post-acute coronary syndrome: the IMPROVE-IT trial. J Am Coll Cardiol. 2016;67(4):353-361. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
