

How to reduce cisatracurium consumption in ARDS patients: the TOF-ARDS study
- PMID: 28770545
- PMCID: PMC5540745
- DOI: 10.1186/s13613-017-0305-2
How to reduce cisatracurium consumption in ARDS patients: the TOF-ARDS study
Abstract
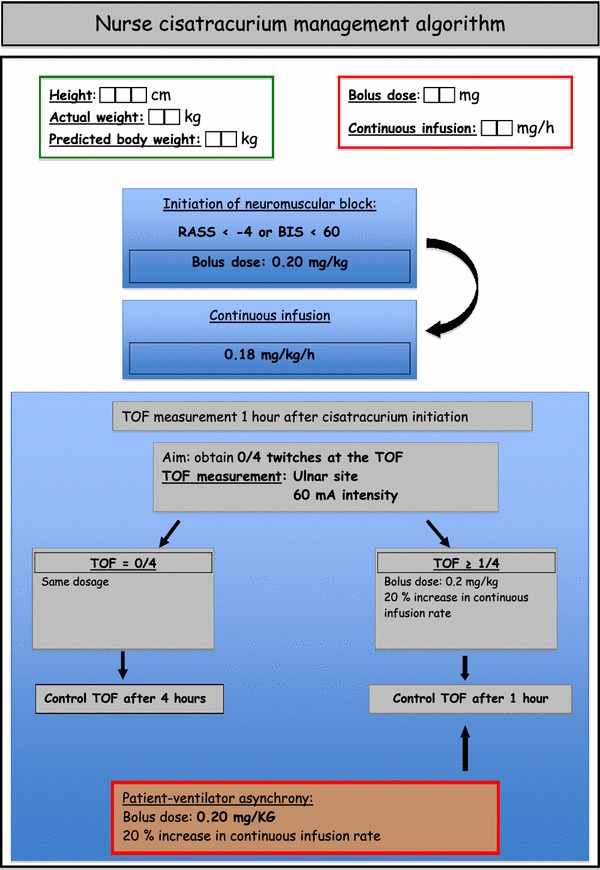
Background: Neuromuscular blocking agents (NMBAs) have been shown to improve the outcome of the most severely hypoxemic, acute respiratory distress syndrome (ARDS) patients. However, the recommended dosage as well as the necessity of monitoring the neuromuscular block is unknown. We aimed to evaluate the efficiency of a nurse-directed protocol of NMBA administration based on a train-of-four (TOF) assessment to ensure a profound neuromuscular block and decrease cisatracurium consumption compared to an elevated and constant dose regimen. A prospective open labeled study was conducted in two medical intensive care units of two French university hospitals. Consecutive ARDS patients with a PaO2/FiO2 ratio less than 120 with a PEEP ≥5 cm H2O were included. Cisatracurium administration was driven by the nurses according to an algorithm based on TOF monitoring. The primary endpoint was cisatracurium consumption. The secondary endpoints included the quality of the neuromuscular block, the occurrence of adverse events, and the evolution of ventilatory and blood gas parameters.
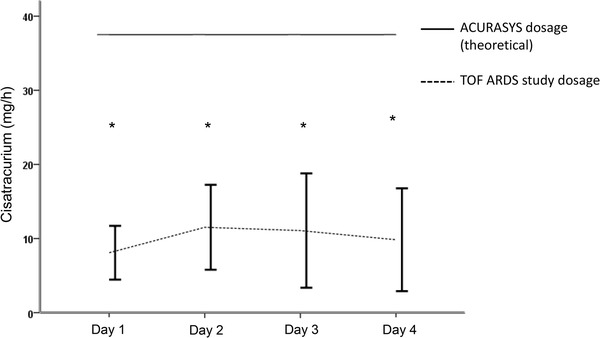
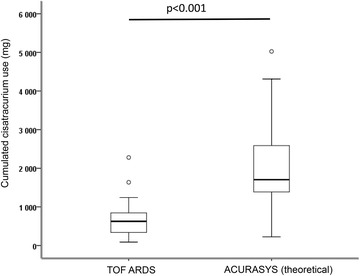
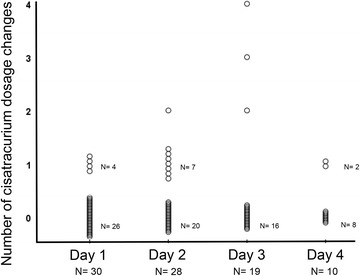
Results: Thirty patients were included. NMBAs were used for 54 ± 30 h. According to this new algorithm, the initial dosage of cisatracurium was 11.8 ± 2 mg/h, and the final dosage was 14 ± 4 mg/h, which was significantly lower than in the ACURASYS study protocol (37.5 mg/h with a constant infusion rate (p < 0.001). The overall cisatracurium dose used was 700 ± 470 mg in comparison with 2040 ± 1119 mg for patients had received the ACURASYS dosage for the same period (p < 0.001). A profound neuromuscular block (TOF = 0, twitches at the ulnar site) was obtained from the first hour in 70% of patients. Modification of the cisatracurium dosage was not performed from the beginning to the end of the study in 60% of patients. Patient-ventilator asynchronies occurred in 4 patients.
Conclusion: A nurse-driven protocol based on TOF monitoring for NMBA administration in ARDS patients was able to decrease cisatracurium consumption without significantly affecting the quality of the neuromuscular block.
Keywords: ARDS; Cisatracurium; Cost; Neuromuscular blockers; Train-of-four.
Figures
References
-
- Network Acute Respiratory Distress Syndrome, Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301–1308. doi: 10.1056/NEJM200005043421801. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
