

Effect of frequency of clinic visits and medication pick-up on antiretroviral treatment outcomes: a systematic literature review and meta-analysis
- PMID: 28770599
- PMCID: PMC6192466
- DOI: 10.7448/IAS.20.5.21647
Effect of frequency of clinic visits and medication pick-up on antiretroviral treatment outcomes: a systematic literature review and meta-analysis
Abstract
Introduction: Expanding and sustaining antiretroviral therapy (ART) coverage may require simplified HIV service delivery strategies that concomitantly reduce the burden of care on the health system and patients while ensuring optimal outcomes. We conducted a systematic review to assess the impact of reduced frequency of clinic visits and drug dispensing on patient outcomes.
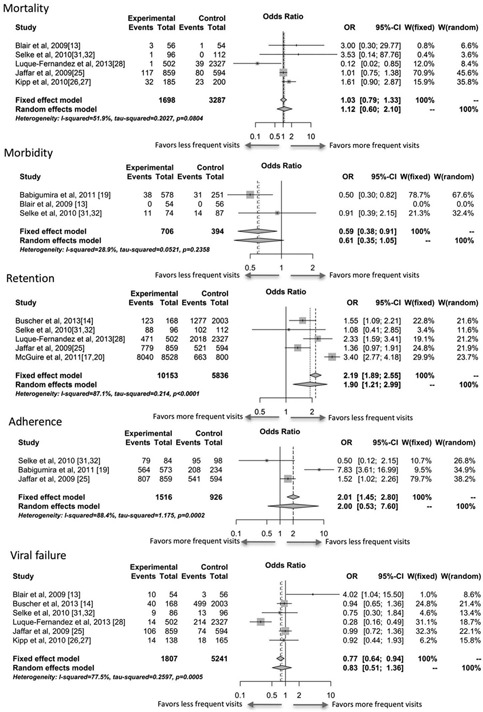
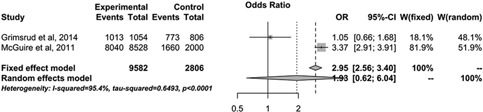
Methods: As part of the development process of the World Health Organization antiretroviral (ARV) guidelines, we systematically searched medical literature databases for publications up to 30 August 2016. Information was extracted on trial characteristics, patient characteristics and the following outcomes: mortality, morbidity, treatment adherence, retention, patient and provider acceptability, cost and patients exiting the programme. When feasible, conventional pairwise meta-analyses were conducted. Results and discussion Of 6443 identified citations, 21 papers, pertaining to 16 studies, were included in this review, with 11 studies contributing to analyses. Although analyses were feasible, they were limited by the sparse evidence base, despite the importance of the research area, and relatively low quality. Comparative analyses of eight studies reporting on frequency of clinic visits showed that less frequent clinic visits led to higher odds of being retained in care (odds ratio [OR]: 1.90; 95% CI: 1.21-2.99). No differences were found with respect to viral failure, morbidity or mortality; however, most estimates were favourable to reduced clinic visits. Reduced frequency of ARVs pick-ups showed a trend towards better retention (OR: 1.93; 95% CI: 0.62-6.04). Strategies using community support tended to have better outcomes; however, their implementation varied, particularly by location. External validity may be questionable.
Conclusions: Our systematic review suggests that reduction of clinical visits (and likely ARVs pick-ups) may improve clinical outcomes, and that they are a viable option to relieve health systems and reduce burden of care for PLHIV. Strategies aimed at reducing clinic visits or drug refill services should focus on stable patients who are virally suppressed, tolerant to their drug regimen and fully adherent. These strategies may be critical to the current changes taking place in HIV treatment policy; thus, due to the data limitations, further high quality research is needed to inform policy and programmatic interventions.
Keywords: HIV Services; clinical visit frequency; antiretroviral therapy HIV/AIDS; systematic literature review; meta-analysis.
Conflict of interest statement
We declare that we have no conflicts of interest.
Figures

References
-
- UNAIDS . “15 by 15”. A global target achieved. Geneva: UNAIDS; 2015.
-
- Kranzer K, Ford N. Unstructured treatment interruption of antiretroviral therapy in clinical practice: a systematic review. Trop Med Int Health. 2011;16(10): 1297–313. - PubMed
-
- IeDEA‐WHO Collaboration: global analysis of retention in care in initial HIV care and treatment programmes in the IeDEA regions . 2015.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
