

Association of Mismatch Repair Mutation With Age at Cancer Onset in Lynch Syndrome: Implications for Stratified Surveillance Strategies
- PMID: 28772289
- PMCID: PMC5824283
- DOI: 10.1001/jamaoncol.2017.0619
Association of Mismatch Repair Mutation With Age at Cancer Onset in Lynch Syndrome: Implications for Stratified Surveillance Strategies
Abstract
Importance: Lynch syndrome is caused by dominantly inherited germline mutations that predispose individuals to colorectal, endometrial, ovarian, and other cancers through inactivation of the cellular mismatch repair system. Lynch syndrome–associated cancers are amenable to surveillance strategies that may improve survival. The age at which surveillance should start is disputed.
Objective: To determine whether mutated gene and type of mutation influence age at onset of Lynch syndrome–associated cancers.
Design, setting, and participants: A retrospective cohort study of individuals with Lynch syndrome–associated colorectal, endometrial, and/or ovarian cancers whose medical records were included in the clinical database of a large quaternary referral center for genomic medicine in the Northwest of England.
Exposures: Mutated gene (MLH1, MSH2, MSH6, and/or PMS2) and type of mutation (truncating, splicing, or large rearrangement).
Main outcomes and measures: Age at cancer diagnosis.
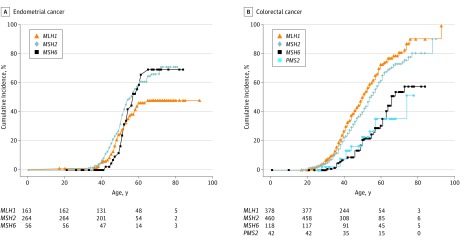
Results: A total of 1063 individuals with proven Lynch syndrome were included, 495 male and 568 female (mean age 52 years; age range, 10-93 years [children were included in the database, but no children developed cancer]). There were 546 men and women with colorectal cancer, 162 women with endometrial cancer, and 49 women with ovarian cancer; mean follow-up was 68.2 months. Among MLH1 mutation carriers, mutations in MLH1 were associated with colorectal cancer in 249 (61%) of 409 men and women; endometrial cancer in 53 of 196 (27%) women; and ovarian cancer in 15 (8%) of 196 women. Among MSH2 mutation carriers, mutations in MSH2 (the most prevalent mutations overall) were most commonly associated with female-specific cancers: endometrial cancer in 83 (30%) of 279 women; ovarian cancer in 28 (10%) of 279 women; and colorectal cancer in 239 (50%) 479 men and women. Mutations in MSH6 were less prevalent, and MSH6 mutation carriers presented with colorectal and endometrial cancer at later ages than carriers of mutations in MSH2 or MLH1. When stratified by mutation type, women with truncating MLH1 mutations had later ages of onset of endometrial cancer than those with nontruncating mutations (median difference, 6.6 years; 95% CI, 2.7-10.4; P = .002). Carriers of truncating MLH1 mutations presented with colorectal cancer at later ages than those with other mutations, but the difference was not statistically significant.
Conclusions and relevance: Individuals with known Lynch syndrome could be risk stratified by mutated gene and mutation type in tailored surveillance programs. Specifically, individuals with MSH6 mutations could be offered cancer surveillance from a later age. Furthermore, those with truncating MLH1 mutations could begin endometrial cancer surveillance later than those with nontruncating mutations.
Conflict of interest statement
Figures
Comment in
-
Findings Linking Mismatch Repair Mutation With Age at Endometrial and Ovarian Cancer Onset in Lynch Syndrome-Reply.JAMA Oncol. 2018 Jun 1;4(6):890-891. doi: 10.1001/jamaoncol.2018.0280. JAMA Oncol. 2018. PMID: 29621375 No abstract available.
-
Findings Linking Mismatch Repair Mutation With Age at Endometrial and Ovarian Cancer Onset in Lynch Syndrome.JAMA Oncol. 2018 Jun 1;4(6):889. doi: 10.1001/jamaoncol.2018.0253. JAMA Oncol. 2018. PMID: 29621388 No abstract available.
-
Findings Linking Mismatch Repair Mutation With Age at Endometrial and Ovarian Cancer Onset in Lynch Syndrome.JAMA Oncol. 2018 Jun 1;4(6):889-890. doi: 10.1001/jamaoncol.2018.0256. JAMA Oncol. 2018. PMID: 29621391 No abstract available.
References
-
- Lynch HT, Lynch JF. What the physician needs to know about Lynch syndrome: an update. Oncology (Williston Park). 2005;19(4):455-463. - PubMed
-
- Mecklin JP, Järvinen HJ. Surveillance in Lynch syndrome. Fam Cancer. 2005;4(3):267-271. - PubMed
-
- Mesher D, Dove-Edwin I, Sasieni P, et al. A pooled analysis of the outcome of prospective colonoscopic surveillance for familial colorectal cancer. Int J Cancer. 2014;134(4):939-947. - PubMed
-
- Auranen A, Joutsiniemi T. A systematic review of gynecological cancer surveillance in women belonging to hereditary nonpolyposis colorectal cancer (Lynch syndrome) families. Acta Obstet Gynecol Scand. 2011;90(5):437-444. - PubMed
-
- Rosenthal AN, Fraser L, Philpott S, et al. Final results of 4-monthly screening in the UK Familial Ovarian Cancer Screening Study (UKFOCSS Phase 2). J Clin Oncol. 2013;31(suppl):abstr 5507.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
